Tadalafil zeigt eine konstante Resorption im Gastrointestinaltrakt, mit maximalen Plasmaspiegeln nach rund zwei Stunden. Der Wirkstoff verteilt sich gut im Gewebe und weist eine hohe Plasmaproteinbindung auf. Seine lange Halbwertszeit erlaubt eine verlängerte Wirkphase. Der Metabolismus erfolgt über das hepatische Enzymsystem CYP3A4, mit der Bildung inaktiver Metaboliten. Exkretion geschieht primär über den Stuhl. Die Häufigkeit von Nebenwirkungen steigt mit der Dosis, wobei vor allem vasodilatatorische Effekte dominieren. Ein gängiger Bezugspunkt in pharmakologischen Analysen ist cialis ohne rezept, das mit dieser Wirkstoffklasse assoziiert ist.
Untitled
November 2012 PRINTER-FRIENDLY VERSION AT RHEUMATOLOGYPRACTICENEWS.COM
Rheumatology Practice News SPECIAL EDITION
SOUMYA D. CHAKRAVARTY, MD, PHD Fellow in Rheumatology, Hospital for Special Surgery; Clinical Fellow in Medicine, Weill Cornell Medical College, New York, New YorkAll rights r STEPHEN A. PAGET, MD, FACP, FACR Copyright 2012 McMahon Publishing Gr Physician-in-Chief Emeritus, Department of Medicine, Division of Rheumatology, Hospital for Special Surgery; Professor of Medicine, Department of Medicine, Weill Cornell Medical College, New York, New Yorkeserved. Repr Dr. Paget has served as an advisor or consultant for Crescendo Bioscience, Inc., and Medscape. Dr. Chakravarty reported no relevant financial conflicts.
Ankylosing spondylitis (AS) is a term derived
oduction in whole or in part without permission is pr
from the Greek roots ankylos or “bent” (modern
implications being fusion or adhesions), and
spondylos or “vertebral disk.” A chronic inflammatory
disease, AS predominantly affects the axial skeleton,
specifically the spine and sacroiliac joints. It is the
classic prototypical member of a large and broader
oup unless otherwise noted.
family of disease states termed spondyloarthritides
(SpA), which include psoriatic arthritis, reactive
arthritis, spondylitis and arthritis associated with
inflammatory bowel disease, and undifferentiated SpA.
eral clinical and genetic features, sive cumulative joint damage, defor-
among them being axial skeletal mity, extraarticular manifestations, cess driven by the activity of T or B
ric oligoarthritis with dactylitis and cause.
ohibited. xamining disease concor-
ifestations, such as anterior uveitis; Pathogenesis of AS
AS is known to be a chronic immunologic disorders, in which genetic association with AS is that
of HLA-B27. In particular, AS is gen-
immune-mediated inflammatory a hereditary component (such as of HLA-B27, with its association first
young adulthood between ages 20 gin remains to be fully elucidated. matory response appear to propel overall contribution to the herita-and 30 years, with men being slightly
Initially, the identification of HLA-B27 as a factor in the development
and 10 years.2 Understanding the dominance, or an association with geting T-cell co-stimulation using role for autoreactive CD8-positive underlying pathogenesis of AS, iden-
disease-specific autoantibodies. abatacept (Orencia, Bristol-Myers T cells. In this model, an “arthrito-
tifying its clinical features early in the
ing early, aggressive therapy may be driven primarily by an innate Genentech), an anti-CD20 monoclo-
immune response triggered by nal antibody used in the treatment
November 2012
Rheumatology Practice News SPECIAL EDITION
Table 1. ASAS HLA-B27), roles played by other pro-
Classification Criteria
teins such as E-cadherin and α E/β7 having demonstrated sacroiliitis on
For Axial SpA Sacroiliitis on imaging plus 1 or more SpA feature OR Classification of Disease HLA-B27-positive plus 2 or more SpA features
AS typically are used for research SpA.26
SpA features: All rights r
become incorporated into clinical cohort of patients (where the pre-
practice. The modified New York test probability of having axial SpA
Copyright 2012 McMahon Publishing Gr
are the most widespread. Under a sensitivity of 82.9% and specific-
eserved. Repr HLA-B27 with AS, less than 1 in 20
HLA-B27-positive individuals will
met.24 The clinical criteria include purposes in clinical practice, in the
nal mobility, and restricted chest they may help physicians make an
oduction in whole or in part without permission is pr
likelihood of a HLA-B27-positive car-
Unfortunately, the mNY criteria festations of SpA only (but that later
tions. One of these, ERAP1 (endoplas-
ASAS, Assessment of SpondyloArthritis
international Society; CRP, C-reactive
protein; NSAID, nonsteroidal anti-inflam-
matory drug; SpA, spondyloarthritides
endoplasmic reticulum. ERAP1 serves
clinically relevant features, and an dactylitis plus (a) 1 or more of the
emphasis on restrictions in spine following—psoriasis, IBD, anteced-
mobility and chest expansion that ent inf
oup unless otherwise noted. ection, HLA-B27, uveitis, sac- Clinical Features and Diagnosis
suggests that dysfunctional antigen has considerable heterogeneity but
following: inflammatory back pain, graphic disease often lags behind SpA.27
Another contributor appears oligoarthritis of the lower extrem-
to be the interleukin (IL)-17–IL-23 ities predominantly, dactylitis, by as much as 10 years.25 There-
Imaging in AS
extraarticular manifestations such classifying definite cases of AS but
receptor (IL-23R) gene associated as apical pulmonary fibrosis, aor-
tic insufficiency, heart block, uveitis,
sis and IBD.16-18 IL12B, which encodes
To better enable clinicians in with AS. Indeed, the presence of
component of the IL-12 and IL-23 to a well-established paradigm of identifying those patients with early
ohibited.
receptors, also has been linked to the “joint-gut axis,” with prevalence
It should be noted that more ranging from 16% to 33% and involve-
express HLA-B27.20 These patients a feature of SpA in about 70% of oped classification criteria for axial
generally have clinical symptoms patients (7% to 12% of patients with
SpA—which encompasses patients the annulus fibrosus (the Sharpey’s
similar to those who are positive SpA develop overt IBD over the long
with chronic back pain who have fibers), also can be seen on spine
for HLA-B27, except for a later age
tion with any HLA gene has been IBD, with a much larger number of history, and responsiveness to non-
steroidal anti-inflammatory drugs sions and sclerosis. Coupled with
patients with AS, although IL-23R
and IL-12B have been found to be copy or by histologic findings.23 A
The criteria can be fulfilled damage before detection of disease,
shared etiology between IBD and through 1 of 2 pathways: by imag-
tive of a patient’s HLA-B27 status, SpA (including idiopathic AS) is ing or clinical, although both require
thought to exist and includes the the presence of chronic back pain iac joints and spine increasingly has
presence of the HLA-B27 gene (25%
(≥3 months) and onset of symptoms been adopted to evaluate patients
November 2012
Rheumatology Practice News SPECIAL EDITION
Table 2. BASDAI Each of the following rated by the patient on a scale of 0 to 10: Treatment of AS
over the years, beginning with a trial of 2 or more NSAIDs over
All rights r
sists despite NSAID therapy—as measured by an elevated
Copyright 2012 McMahon Publishing Gr
scores from 1 to 4) + (Sum of scores from 5 to 6)/2
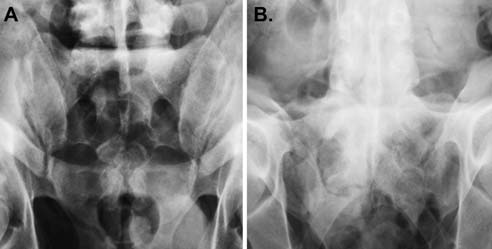
Figure 1. Pelvic radiographs demonstrating varying stages of sacroiliitis. A. Mild BASDAI, Bath Ankylosing Spondylitis eserved. Repr
irregularity in both sacroiliac joints with minimal subcortical sclerosis and slight
subligamentous erosive change on the right. B. Fusion of the sacroiliac joints, as
well as bridging syndesmophytes in the lower lumbar spine.
apy.34,35 Of note, nonbiologic disease-modifying antirheu-
who are thought to have clinically Accurate quantification also empow-
matic drugs (DMARDs), such been extended to establishing effi-
ers the clinician to assess response as methotrexate, sulfasalazine, and cacy in nonradiographic axial SpA
oduction in whole or in part without permission is pr
radiographs would otherwise be to current therapy and determine leflunomide, have not proven effica-
patients. In the first such clinical trial,
axial inflammation compared with used, the most common being the
infliximab (Remicade, Centocor), for 12 weeks, followed by an open-
MRI sequences, the fluid-sensitive ease Activity Index (BASDAI). This etanercept (Enbrel, Amgen/Pfizer), label extension that continued up to short-tau inversion recovery (STIR)
straightforward scoring system is adalimumab (Humira, Abbott Labo-
patient-driven and consists of 6 ratories), and golimumab (Simponi,
oup unless otherwise noted.
TNF agents in axial SpA first was (P=0.004). After switching to adali-
demonstrated in studies enrolling mumab, a similar degree of efficacy
ered the most significant finding score has a range of 0 to 10, with a
of active inflammation in AS, and score of 4 or greater indicating high
ohibited.
treated patients (P=0.033).37 Signif-icantly more lesions resolved in the
Assessment of Disease
infliximab group (P<0.001), whereas
Activity in AS Figure 2. MRI (T2-weighted imaging) showing osseous fusion of the
imaged portions of the sacroiliac joints bilaterally, reflecting bony ankylo-
sis. Black arrows indicate bone marrow edema, reflecting ongoing active
November 2012
Rheumatology Practice News SPECIAL EDITION
Table 3. Current Therapeutic Recommendations in AS (with fulfillment of the ASAS criteria for axial SpA)
kopf-1 (DKK-1), an inhibitor of the Wnt
DKK-1 has been associated with higher
with osteopenia.48 DKK-1 has been
All rights r Copyright 2012 McMahon Publishing Gr AS, ankylosing spondylitis; ASAS, Assessment of SpondyloArthritis international Society; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; COX, cyclooxygenase; DMARD, disease-modifying antirheumatic drug; TNF, tumor necrosis factor eserved. Repr
48 was significantly larger (P=0.02)
Predicting Response oduction in whole or in part without permission is pr
some specific positive predictors of after 3 months of therapy.50 Serum
response to treatment. The first is short
levels of DKK-1 were significantly
between baseline and 48 weeks, years for all treatment groups.39
controls (P<0.0001), whereas lev-
10 years have had better responses els of osteocalcin and osteopro-
in the sulfasalazine group (P=0.04),
reduced spinal inflammation of AS more than 10 years.42 Second, young
(P<0.0001).50 However, serum lev-
and 50% of patients treated with detected on MRI. Improvements were
tor of good response—the highest after 3 months of anti-TNF therapy,
oup unless otherwise noted. eas osteocalcin significantly
increased (P<0.0001) and osteopro-
Recently published results from lowed by those in the 30- to 39-year-
graphic and nonradiographic) are treatment of nonradiographic axial
levels of DKK-1 in AS patients con-
under way. Recently published SpA.41 The study included patients
umab—A Randomized Study in teria for axial SpA, had a BASDAI of
Ankylosing Spondylitis Subjects at least 4, a total back pain score of
Another active area of current undergoing longer durations of anti-
cacy and safety of golimumab in meeting mNY criteria for AS were spe-
damage in patients with AS, with a explanation for the inability of anti-
ohibited.
Patients were randomized to as spinal ankylosis has the highest of new bone despite tangible symp-
with active AS were randomly either adalimumab 40 mg every effect on long-term spinal immobility
and disability. It has been previously with AS.
tions of placebo, golimumab 50 cantly more patients in the adalim-
weeks.39 After 16 weeks, patients weeks than those receiving placebo desmophytes, as measured by a scor-
(36% vs 15%; P<0.001) and signifi-
ing system termed the modified Stoke Ankylosing Spondylitis Spinal Score
(if originally on placebo) or 100 mg (if
ent protective effects of NSAIDs is appears to have no meaningful effi-
sacroiliac joints on MRI significantly thought to be due not to their anti-
concluded that adalimumab has a ity through the downregulation of imab and abatacept in AS also has
progression in patients with AS has cacy of rituximab in patients with
November 2012
Rheumatology Practice News SPECIAL EDITION
NSAID-refractory AS who either 3. Burn GL, Svensson L, Sanchez-Blanco
spondyloarthritis. Ann Rheum Dis.
early sacroiliitis. Arthritis Rheum. 2009;60(4):946-954.
Dekker-Saeys AJ, Keat AC. Follow-up study
for autoimmune disease? FEBS Lett.
of ankylosing spondylitis over a period of 12
38. Song IH, Hermann K, Haibel H, et al.
years (1977-1989). Scand J Rheumol Suppl.
Effects of etanercept versus sulfasalazine
in early axial spondyloarthritis on active
classifi cation of the immunological diseases.
22. Brakenhoff LK, van der Heijde DM, Hommes
DW, Huizinga TW, Fidder HH. The joint-gut
randomised controlled trial. Ann Rheum Dis.
Song IH, Heldmann F, Rudwaleit M, et al.
Treatment of active ankylosing spondylitis
J Crohns Colitis. 2010;4(3):257-268.
with abatacept: an open-label, 24-week pilot
39. Braun J, Deodhar A, Inman RD, et al.
study. Ann Rheum Dis. 2011;70(6):1108-1110.
spondylitis and bowel disease. Best Pract
every 4 weeks in ankylosing spondylitis:
Song IH, Heldmann F, Rudwaleit M, et al.
Res Clin Rheumatol. 2006;20(3):451-471.
Different response to rituximab in tumor
24. van der Linden S, Valkenburg HA, Cats
Ann Rheum Dis. 2012;71(5):661-667.
necrosis factor blocker-naive patients with
A. Evaluation of diagnostic criteria for
40. Braun J, Baraliakos X, Hermann KG, et al.
All rights r
active ankylosing spondylitis and in patients
modifi cation of the New York criteria.
Golimumab reduces spinal infl ammation in
have failed: a twenty-four-week clinical trial.
Arthritis Rheum. 1984;27(4):361-368.
ankylosing spondylitis: MRI results of the
Copyright 2012 McMahon Publishing Gr Arthritis Rheum. 2010;62(5):1290-1297.
25. Mau W, Zeidler H, Mau R, et al. Clinical
study. Ann Rheum Dis. 2012;71(6):878-884.
possible ankylosing spondylitis. Results
spondylitis in twins: the role of genes, HLA,
of a 10-year followup. J Rheumatol.
et al. Effi cacy and safety of adalimumab
eserved. Repr
and the environment. Arthritis Rheum.
spondyloarthritis: results of a randomised
26. Rudwaleit M, van der Heijde D, Landewe
placebo-controlled trial (ABILITY-1). Ann Rheum Dis. 2012 Jul 7 [Epub ahead of print].
Recurrence risk modelling of the genetic
susceptibility to ankylosing spondylitis. Ann
Society classifi cation criteria for axial
42. Rudwaleit M, Listing J, Brandt J, Braun
Rheum Dis. 2000;59(11):883-886.
J, Sieper J. Prediction of a major clinical
and fi nal selection. Ann Rheum Dis.
of ankylosing spondylitis. Brief Funct oduction in whole or in part without permission is pr
ankylosing spondylitis. Ann Rheum Dis. Genomics. 2011;10(5):249-257.
27. Rudwaleit M, van der Heijde D, Landewe R,
et al. The Assessment of SpondyloArthritis
Hermann E, Yu DT, Meyer zum Buschenfelde
43. Wanders A, Heijde D, Landewe R, et al.
KH, Fleischer B. HLA-B27-restricted CD8 T
International Society classifi cation criteria
Nonsteroidal antiinfl ammatory drugs reduce
cells derived from synovial fl uids of patients
for peripheral spondyloarthritis and for
radiographic progression in patients with
spondyloarthritis in general. Ann Rheum Dis. 2011;70(1):25-31.
ankylosing spondylitis: a randomized clinical
spondylitis. Lancet. 1993;342(8872):646-650.
trial. Arthritis Rheum. 2005;52(6):1756-1765.
May E, Dorris ML, Satumtira N, et al. CD8
Maksymowych WP. The impact of MRI on the
Prostaglandins in bone: bad cop, good cop?
the pathogenesis of arthritis or colitis
clinical management of infl ammatory arthritides. Skeletal Radiol. 2011;40(9):1153-
Trends Endocrinol Metab. 2010;21(5):294-
in HLA-B27 transgenic rats. J Immunol.
45. van der Heijde D, Landewe R, Baraliakos X,
et al. Radiographic fi ndings following two
utility of MRI in early spondyloarthritis. Curr oup unless otherwise noted. Rheumatol Rep. 2011;13(5):402-408.
years of infl iximab therapy in patients with
beta2-microglobulin-transgenic rats is not
ankylosing spondylitis. Arthritis Rheum.
prevented by lack of CD8. Arthritis Rheum.
Sieper J, Schöntube M, Braun J. Very early
46. van der Heijde D, Landewe R, Einstein S, et
spondyloarthritis: where the infl ammation in
Conclusion
al. Radiographic progression of ankylosing
the sacroiliac joints starts. Arthritis Rheum.
treatment with etanercept. Arthritis Rheum.
response augment interleukin-23 production
in transgenic rats. Arthritis Rheum.
47. van der Heijde D, Salonen D, Weissman
in sacroiliac joints enhances diagnostic
utility of magnetic resonance imaging in
with ankylosing spondylitis treated with
Jongh BM, Cats A. The risk of developing
early spondylarthritis. Arthritis Care Res. 2010;62(12):1763-1771.
adalimumab for up to 2 years. Arthritis Res
ankylosing spondylitis in HLA-B27 positive
Ther.2009;11(4):R127.
individuals. A comparison of relatives of
32. D’Agostino MA. Role of ultrasound in the
diagnostic work-up of spondyloarthritis.
emerging role of Dickkopf-1 in bone biology:
population. Arthritis Rheum. 1984;27(3):241-
Curr Opin Rheumatol. 2012;24(4):375-379.
is it the main switch controlling bone and
joint remodeling? Semin Arthritis Rheum.
Yan J, Parekh VV, Mendez-Fernandez Y, et
ohibited.
al. In vivo role of ER-associated peptidase
approach to defi ning disease status in
49. Uderhardt S, Diarra D, Katzenbeisser J, et
activity in tailoring peptides for presentation
ankylosing spondylitis: the Bath Ankylosing
by MHC class Ia and class Ib molecules. J
al. Blockade of Dickkopf (DKK)-1 induces
Exp Med. 2006;203(3):647-659. J Rheumatol. 1994;21(12):2286-2291.
fusion of sacroiliac joints. Ann Rheum Dis.
34. Braun J, van den Berg R, Baraliakos X,
50. Kwon SR, Lim MJ, Suh CH, et al. Dickkopf-1
level is lower in patients with ankylosing
identifi es autoimmunity variants. Nat Genet.
of ankylosing spondylitis. Ann Rheum Dis.
spondylitis than in healthy people and is not
infl uenced by anti-tumor necrosis factor therapy. Rheumatol Int. 2012;32(8):2523-
35. van der Heijde D, Sieper J, Maksymowych
WP, et al. 2010 Update of the international
Haibel H, Rudwaleit M, Listing J, Sieper
identifi cation of IL23R as psoriasis-risk
J. Open label trial of anakinra in active ankylosing spondylitis over 24 weeks. Ann
spondyloarthritis. Ann Rheum Dis. Rheum Dis. 2005;64(2):296-298. References
36. Haibel H, Rudwaleit M, Listing J, et al.
genome-wide association study identifi es
Effi cacy of adalimumab in the treatment
IL23R as an infl ammatory bowel disease
Braun J, Sieper J. Ankylosing spondylitis.
gene. Science. 2006;314(5804):1461-1463.
radiographically defi ned sacroiliitis: results
Lancet. 2007;369(9570):1379-1390.
Evans DM, Spencer CC, Pointon JJ, et al.
of a twelve-week randomized, double-blind,
Interaction between ERAP1 and HLA-B27 in
ankylosing spondylitis implicates peptide
open-label extension up to week fi fty-two.
Ann Rheum Dis. 2008;58(7):1981-1991.
in disease susceptibility. Nature Genet.
with ankylosing spondylitis. Rheumatol Int.
Clinical and imaging effi cacy of infl iximab
CURRICULUM VITAE PATRICK JOHN RIEDEL, M.D. WORK ADDRESS: TELEPHONE: MEDICAL LICENSURE: BOARD CERTIFICATION: EDUCATION: Glaucoma Fellowship, University of Utah John Moran Eye Center, Salt Lake City, Utah Ophthalmology Residency, University of Iowa Hospital and Clinics, Iowa City, Iowa Hennepin County Medical Center, Minneapolis, Minnesota University of M
Een kort verhaal door Marnix van Rijswijk Emma, zeventien jaar keek in de spiegel en wreef over haar zwangere buik, maar niet op de warme en trotse manier zoals een toekomstige moeder doet. Nee, ze wreef ruw en koud over haar buik alsof ze er een vlek af wou poetsen. Nu was het ook echt zichtbaar. Ze kon er niet meer omheen, zichzelf niet meer voor de gek houden dat ze niet zwanger was. Ze d
 November 2012
November 2012 
 November 2012
November 2012






 November 2012
November 2012 

 November 2012
November 2012