Tadalafil zeigt eine konstante Resorption im Gastrointestinaltrakt, mit maximalen Plasmaspiegeln nach rund zwei Stunden. Der Wirkstoff verteilt sich gut im Gewebe und weist eine hohe Plasmaproteinbindung auf. Seine lange Halbwertszeit erlaubt eine verlängerte Wirkphase. Der Metabolismus erfolgt über das hepatische Enzymsystem CYP3A4, mit der Bildung inaktiver Metaboliten. Exkretion geschieht primär über den Stuhl. Die Häufigkeit von Nebenwirkungen steigt mit der Dosis, wobei vor allem vasodilatatorische Effekte dominieren. Ein gängiger Bezugspunkt in pharmakologischen Analysen ist cialis ohne rezept, das mit dieser Wirkstoffklasse assoziiert ist.
Pii: s0306-4530(99)00025-6
Psychoneuroendocrinology 24 (1999) 727 – 741
Two weeks of transdermal estradiol treatment
in postmenopausal elderly women and its effect
on memory and mood: verbal memory changes
are associated with the treatment induced
Oliver T. Wolf a,b,c, Brigitte M. Kudielka a,
Dirk H. Hellhammer a, Sonja To¨rber a, Bruce S. McEwen b,
a Center for Psychobiological and Psychosomatic Research, Uni6ersity of Trier, Dietrichstraße 10-11,
b Laboratory of Neuroendocrinology, Rockefeller Uni6ersity, New York, NY, USA
c Neuroimaging Laboratory, Department of Psychiatry, NYU School of Medicine, New York, NY, USA
Received 18 December 1998; accepted 12 April 1999
Abstract
The present randomized double blind study investigated the effects of a 2 week transder-
mal estradiol treatment on memory performance in 38 healthy elderly women. Cognitiveperformance was tested at baseline and after 2 weeks of estradiol or placebo treatment usingverbal, semantic, and spatial memory tests as well as a mental rotation task and the Stroop. Initial results showed no differences after treatment between placebo or estradiol treatedsubjects. However, within treatment group analysis revealed that estradiol treated subjectswho reached higher estradiol levels (larger than 29 pg/ml) performed significantly better aftertreatment in the delayed recall of the paired associate test (verbal memory) than subjects who
* Corresponding author. Tel.: + 49-651-975-8624; fax: + 49-651-975-8640.
0306-4530/99/$ - see front matter 1999 Elsevier Science Ltd. All rights reserved. PII: S 0 3 0 6 - 4 5 3 0 ( 9 9 ) 0 0 0 2 5 - 6
O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
reached lower estradiol levels (P B0.05). A nonsignificant trend was observed for theimmediate recall condition (P B0.10) These findings were strengthened by correlationsbetween treatment-induced estradiol levels and changes in verbal memory performance. Inaddition, there was an association between estradiol levels and mood changes. Howevermood changes were not significantly associated with changes in verbal memory performance(P \0.20). The present study supports the idea that estradiol replacement has specific effectson verbal memory in healthy postmenopausal women, with delayed recall being moreaffected. It suggests that these effects can occur relatively rapidly, and that there may be adose response relationship of estradiol to memory enhancement. Furthermore, the fact thatthese results were obtained in women who had been menopausal for an average of 17 yearsbefore entering the study indicates that the brain maintains a sensitivity for estrogens evenafter years of low estradiol plasma concentrations. 1999 Elsevier Science Ltd. All rightsreserved. Keywords: Estradiol; Menopause; Replacement; Memory; Aging; Humans
1. Introduction
In recent years there is growing interest in the effects of estradiol on the central
nervous system (CNS). Animal studies have shown multiple sites of estradiol actionin brain areas which are involved in memory processes (McEwen et al., 1995, 1997;McEwen and Alves, in press), including the forebrain as a relevant structure forworking memory (West, 1996; Owen, 1997) and the hippocampus as an importantstructure for declarative (explicit) memory (Eichenbaum et al., 1992; Squire, 1992). Estradiol influences four major forebrain neurochemical systems with widespreadprojections and influences: the basal forebrain cholinergic system, the midbrainserotonergic system, the brainstem noradrenergic system and the midbrain andhypothalamic dopaminergic systems (McEwen et al., 1997, 1995; McEwen andAlves, in press). In the basal forebrain cholinergic system, which is involved inattentional processes (Sarter and Bruno, 1997), estrogen treatment induces cholineacetyltransferase, the enzyme which synthesizes acetylcholine (Luine et al., 1975;Gibbs et al., 1994). In addition estradiol induces synaptic spines in the CA1 regionin the hippocampus, via an interaction with NMDA receptors (Gould et al., 1990;Woolley and McEwen, 1992, 1994; Gazzaley et al., 1996; Woolley et al., 1997). Estradiol also regulates the activity of several neurotrophic factors in the brain (e.g. BDNF; Singh et al., 1995) and NGF and its receptors (see Gibbs et al., 1994).
A few cross-sectional studies reported that women on estradiol replacement
perform better than women without estradiol in verbal tests (Kampen and Sherwin,1994), in name recall (Robinson et al., 1994), in digit span backwards (Carlson andSherwin, 1998) or in several tests of cognitive functions (Kimura, 1995; Jacobs etal., 1998). However, negative findings have also been reported (Barrett-Connor andKritz-Silverstein, 1993). One problem with most of these studies is that estradiollevels were not monitored (Barrett-Connor and Kritz-Silverstein, 1993; Robinson etal., 1994; Kimura, 1995; Jacobs et al., 1998). O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
A more direct approach to investigate possible effects of estradiol on memory
processes is to administer the steroid in an experimental study. More than 40 yearsago Caldwell and Watson (1952) observed that 6 months of estrogen treatmentenhanced verbal memory. Other studies reported estrogen-induced increases incognitive performance on a variety of cognitive functions (Fedor-Freybergh, 1977)or failed to find beneficial effects (Rauramo et al., 1975; Ditkoff et al., 1991;Polo-Kantola et al., 1998). These contradicting results might in part be due todifferent tests used and/or types of estrogen treatment (estradiol versus conjugatedestrogens, which might not achieve high enough estrogen levels in the brain; fordiscussion and review, see: Haskell et al., 1997; Rice et al., 1997; Sherwin, 1997).
In the last decade two placebo controlled studies by Sherwin and colleagues
again reported a specific enhancement of verbal short and long term memory afterestradiol treatment in surgically postmenopausal women (Phillips and Sherwin,1992) or women with low estradiol levels due to pharmacological treatment with aGnRH agonist (Sherwin and Tulandi, 1996), while a third study reported on a moreglobal increase in cognitive function (Sherwin, 1988).
The subjects in the experimental studies by Sherwin and coworkers (Sherwin,
1988; Phillips and Sherwin, 1992; Sherwin and Tulandi, 1996) were all relativelyyoung (mean age below 50) so it remains to be shown whether estradiol can alsoinfluence memory performance in healthy elderly women who had been post-menopausal for several years before being studied. A second important questionconcerns the time and blood levels needed before estradiol effects first appear, sinceall studies published to date tested cognitive performance only several months afterinitiation of hormonal treatment. The present study therefore aimed to investigatethe effects of a 2 week estradiol treatment on verbal and spatial memory perfor-mance in healthy elderly women who had been menopausal for several years, takingcare to relate performance to blood estradiol levels. In addition to the cognitivetests mood was assessed in order to control whether cognitive changes might beassociated with mood changes. 2. Subjects and methods
Forty healthy elderly postmenopausal women, who were recruited by newspaper
advertisements, participated in the experiment. They underwent a comprehensivemedical examination for past or current health problems. Subjects with psychiatric,endocrine, cardiovascular, other chronic diseases, or medicated with psychoactivedrugs, estrogens or glucocorticoids were excluded from participation. Two subjectshad to be excluded from the analysis due to noncompliance with treatment so thatdata from 38 subjects entered data analysis. Subjects had reached menopause since17.4 91.3 years (9S.E.M.) with a range from 7 to 40 years. Thirteen women hadundergone hysterectomy with eight of them having had additional bilateraloophorectomy. Twenty-one subjects (age: 69.5 91.4 years.; body mass index(BMI): 24.45 90.6 kg/m2; years of formal education: 8.4291.0) received estradioltreatment, 17 subjects (age: 67.8 91.2 years.; BMI: 25.190.7 kg/m2; years of
O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
formal education: 8.47 90.6) received placebos. The two groups did not differsignificantly in those descriptive variables (P \20). The study was approved by theethic committee of the University of Trier (Germany) and all subjects gave writteninformed consent.
The study design was placebo controlled and double blind with estradiol or
placebo treatment for 2 weeks. At baseline and after the 2 week treatment periodsubjects, participated in several cognitive tests which covered a broad range ofcognitive functions (see below). Testing was performed in the early afternoon(between 14:00 and 17:00 h). In addition mood was assessed with an adjectivechecklist (see below). Each subject was tested on both appointments by the sameinvestigator.
Subjects received estradiol or placebo patches (Estraderm TTS 100, Geigy, Wehr,
Germany) attached to the subject’s back in a double-blind procedure. The estradiolpatch delivers a mean of 0.1 mg estradiol/day percutaneously over 3 – 4 days. Thesubjects received a total of four patches, and were told to exchange the patch every3.5 days. Reference values provided by the patch manufacturer report averagepatch-induced estradiol levels of 75 pg/ml when a two patch per week treatment isused.
Estradiol levels were measured from baseline and post-treatment blood samples
using a commercially available RIA (Biermann, Bad Nauheim, Germany) with anintra and interassay coefficient below 10%. The two samples from each subject werealways run in the same assay.
Parallel versions of the following cognitive tests were used in a counterbalanced
2.4.1. Semantic memory (6erbal fluency)
Subjects had 1 min to generate as many words as possible to a given first letter,
thereafter a second letter was introduced with another 1 min test period. The totalnumber of produced words was used as test score (Horn, 1983).
2.4.2. Spatial memory (city map task)
Subjects were asked to memorize (within 2 min) a route marked in a city map.
Immediate as well as delayed recall (after the mental rotation task, approximately
O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
10 min later) was assessed by letting the subject draw the learned route into anunmarked map. The number of correctly chosen roads (maximum 31) was used astest score (Baeumler, 1974).
2.4.3. Verbal memory (paired associates)
Six word-pairs of unrelated words were read to the subject (one word per
second). Immediate as well as delayed recall (after the delayed spatial memoryrecall, approximately 10 min later) was tested by presenting the first word of eachpair as a cue. If the subject could not recall the word, the whole pair was read tothe subject again. In each recall condition every pair was tested twice. (Oswald andFleischmann, 1994).
2.4.4. Color word test (Stroop)
The classical version with three cards was used. For each card, the time needed
to read the items (e.g. name the colors on card 2 and 3) was assessed and thedifference between cards 3 and 2 was used as interference score (Stroop, 1935;Oswald and Fleischmann, 1994).
On a piece of paper five copies of a specific letter or number were presented to
the subject. Each item was rotated to different degrees from the normal horizontalposition, in addition one item in each line was flipped horizontally. This item hadto be recognized and crossed out by the subject. The subject was given 2 min tocomplete as many of the 37 presented items as possible (Horn, 1983).
An adjective checklist was used to assess elevated versus depressed mood,
wakefulness versus sleepiness, and calmness versus restlessness. Test scores in thisquestionnaire vary between five and zero with five indicating maximum agreementwith the ‘positive’ end of each scale (Steyer et al., 1994).
After the end of the experiment, subjects were asked to guess what treatment they
Estradiol as well as cognitive data were first analyzed with a two way ANOVA
with the independent factor group (placebo or estradiol) and the repeated measurefactor treatment (pre and post treatment). For the two tests which includedimmediate as well as delayed recall (verbal and spatial memory), analysis were runseparately for the two recall conditions. Data from the estradiol group were furtheranalyzed using an ANOVA with the median split derived group factor high or low
O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
post treatment estradiol levels. In addition, an ANCOVA was calculated with moodchanges as covariates in order to control for possible influences of mood changes onmemory. For all computed ANOVA models post hoc testing was done usingNewman Keuls post hoc test. Pearson product moment correlations between thetreatment induced estradiol levels and changes in cognitive performance or moodwere calculated. In order to further investigate the relationship between estradiol,mood and memory changes a hierarchical regression analyses was performed. Chi-square analysis was used to test whether subjects were able to correctly guesswhat treatment they had received. 3. Results
The estradiol levels are presented in Table 1 ANOVA revealed a significant group
by treatment interaction (F(1,36) = 27.8, P B0.001). Post hoc testing demonstratedthat while both groups did not differ in their estradiol levels before treatment(P \0.20), they differed significantly after treatment (PB0.001).
3.2.1. Comparison between the estradiol and the placebo group
In none of the tests a significant group by treatment interaction could be detect
(all P \0.10), which indicates that the two groups did not differ in their changes ofcognitive performance between the pre treatment and the post treatment session. The actual means for both groups are presented in Table 2. In the verbal memorytest, estradiol treated subjects scored significantly lower than subjects under placebobefore and after treatment in both recall conditions (F(1,36) = 4.5, P B0.05; forboth comparisons), which demonstrates baseline differences in this test between thetwo groups. A practice effect (better performance at the second test day regardlessof treatment) occurred in the verbal fluency task (F(1,36) = 7.1, P B0.01) and in themental rotation task (F(1,36) = 5.3, P B0.05).
Table 1Estradiol levels in subjects receiving estradiol or placebo (mean 9S.E.M.)
a PB0.05 compared to the baseline value. b PB0.05 compared to the placebo group post treatment value. O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
Table 2Memory performance in subjects receiving estradiol or placebo
a Mean9S.E.M. b The placebo group performed better than the estradiol group before and after treatment, which
reflects baseline differences between the two groups in this task.
3.2.2. Within estradiol treatment group comparison between subjects with high6ersus low treatment induced estradiol le6els
There was a large variance in the plasma estradiol levels reached in response to
the skin patch with some subjects showing still relatively low levels after treatment. Therefore, as the next step, the relationship between treatment induced estradiollevels and changes in performance pre and post treatment were investigated withinthe estradiol group. A median split was performed using the median of the estradiolpost treatment level which was 29.3 pg/ml. The three subjects which were closest tothe median were excluded from the analysis, in order to increase the differencebetween the two groups. ANOVA of the estradiol data indicated a significant groupmain effect (F = 31.46, P B0.001) as well as a significant group by treatment
O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
interaction (F = 23.6, P B0.001). Post hoc testing revealed that subjects from thehigh estradiol level group did already had higher estradiol levels at baseline(P B0.05) and in addition showed a much stronger estradiol increase in responseto the treatment. The post treatment levels for the high estradiol group werewithin the physiological range observed in younger women in the follicular phase(Mishell et al., 1971). In contrast, the post treatment levels in the low estradiolgroup were still in the menopausal range and did not differ from the pre treat-ment levels of the high estradiol group. The estradiol levels for both groups arepresented in Table 3. The two groups did not differ significantly in their age,BMI or years or formal education (all P \0.20).
The cognitive data were reanalyzed using this new grouping factor. In the
verbal memory test, the group by treatment interaction tended to be significantfor the immediate recall (F(1,16) = 3.09, P B0.10), and was significant for thedelayed recall (F(1,16) = 6.01, P B0.05). Post hoc testing revealed that, while thegroups did not differ in their performance before treatment, the high increasegroup performed significantly better after treatment (P B0.05; see Fig. 1). Thiseffect was caused by a non significant increase in performance in the highestradiol group in combination with a non significant decrease in performance inthe low estradiol group. In none of the other four cognitive tests was a signifi-cant estradiol increase by treatment interaction observed (all P \0.10). Nearlyidentical results as described above were observed when estradiol increases aftertreatment (delta values), rather than the reached estradiol levels, were used forthe median split (median of estradiol increase: 19 pg/ml).
The relationship between reached estradiol levels and changes in test perfor-
mance (delta values, post treatment test score, minus pre treatment test score)were additionally investigated for the five tests using Pearson’s product momentcorrelations (only for the estradiol treatment group). The results are presented inTable 4. Results indicated a significant correlation between the reached estradiollevels and changes in the delayed verbal memory recall test, while the associationwith the immediate verbal recall test indicated a trend. There was no significantcorrelation between estradiol increases and any of the other four cognitive tests.
Table 3Estradiol levels in subjects from the estradiol treatment group showing low or high treatment inducedestradiol levels
a PB0.05 compared to the baseline value. b PB0.05 compared to the low estradiol group. O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
Fig. 1. Immediate (top) and delayed (bottom) verbal memory performance in women with high versuslow treatment induced estradiol levels in response to the 2 week transdermal estradiol treatment;* P B05 and § PB0.10 in post hoc comparison. The estradiol levels of the two groups are presented inTable 3.
Changes in mood was first compared between the placebo and estradiol treated
women by ANOVA. For none of the three scales a significant group by treatmentinteraction could be detected (all F B1). In a second step, the within groupdifference in the estradiol treated group were investigated by ANOVA, and themedian split derived factor high versus low reached estradiol levels. A significantestradiol increase by treatment interaction was found for the mood factor(F(1,16) = 6.25, P B0.05). Post hoc testing revealed that there was a decrease inmood score in the low estradiol group (from 4.2 90.2 to 3.890.2; PB0.05)between pre and post treatment, while there was no difference in the high estradiol
O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
increase group (4.1 90.1 at both time points). In addition, there was a significantcorrelation between the reached estradiol levels and mood changes (r = 0.52,P B0.05). For the other two scales of the questionnaire, no significant relationshipwith estradiol was observed (neither in the ANOVAs nor in correlational analyses).
3.4. Associations between memory and mood changes
There was a significant association with the treatment induced estradiol increase
for verbal memory as well as for mood. Therefore, we investigated whether thosechanges occurred in parallel. However, changes in memory and mood were notsignificantly correlated (r = 0.22, P = 0.34 for the immediate recall and r = 0.33,P = 0.18 for the delayed recall), although both coefficients tended to show apositive association. To further evaluate this issue, hierarchical regression analysiswas performed. Independent of its entry (as first or as second step) estradiolchanges significantly changed R square (P B0.05), while mood did not (P\0.15)thereby showing that only estradiol changes could explain a significant amount ofthe variance in verbal memory changes. Mood changes were also related to changesin the spatial memory test (r = 0.34, P = 0.13 for the immediate recall and r = 0.48,P B0.05 for the delayed recall). No association was found between mood changesand changes in the other tests.
As a final step, mood was introduced as a covariate in an ANCOVA model to
reanalyze the relationship between the low and high reached estradiol level groupsand delayed recall in the verbal memory test. The group by treatment interactionstayed significant (F = 5.63, P B0.05), thereby demonstrating again that moodchanges could not explain changes in memory.
From one subject treated with placebo no treatment guess was obtained. The
distribution of the guesses is presented in Table 5. Chi square analysis revealed thatthe two groups did not differ significantly from each other (Chi = 0.05, P = 0.80)
Table 4Correlations between the treatment induced estradiol levels and changes in test performance (deltavalues)a
Correlation with treatment induced estradiol levels
a Only subjects from the estradiol treatment group were included into the analysis (n=21)
O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
Table 5Treatment guess in subjects receiving estradiol or placebo treatment
suggesting that subjects were unable to identify the treatment obtained. When onlythe estradiol group was investigated and median split was used as the groupingfactor a similar non significant result was obtained (Chi = 0.22, P = 0.64). 4. Discussion
This study was undertaken to investigate whether a physiological estradiol
replacement dose can exert relatively rapid effects on cognition. While no overalldifference in cognitive performance was observed between placebo and estradioltreatment, a within-treatment-group analysis detected that subjects showing highertreatment induced estradiol levels performed better in the verbal memory test thansubjects showing a less pronounced estradiol increase. These data suggest, there-fore, that estradiol can have rapid and specific effects on verbal memory, as long asreached blood levels are high enough.
It is important to note that the estrogen effects were rather subtle, which is, in
part, reflected in the inability of the subjects to correctly guess the kind of treatmentthey had received. In addition, the effects could only be detected by analyzing theassociations between treatment-induced estradiol levels and changes in memory. Therefore the data should be viewed as preliminary evidence for rapid estradioleffects on memory in normal elderly postmenopausal women. It is noteworthy thatall subjects were healthy elderly women who did not suffer from noticeable memoryproblems. Therefore, strong memory enhancing effects cannot be expected in thispopulation (Sherwin, 1997). One could imagine that longer treatment and/or higherattained estradiol blood levels might also have led to significant changes betweenthe two treatment groups. This needs to be demonstrated in future studies, whichshould monitor the effects of estradiol over a longer treatment period, withcognitive testing being carried at several time points ranging from days to months,if enough parallel versions of the specific tests are available. In addition, futurestudies should consider estradiol treatment in mildly cognitively impaired elderlywomen who show already signs of frontal and hippocampal atrophy or dysfunction(West, 1996; Convit et al., 1997). Such studies could connect the results obtained inhealthy women to the promising data observed in Alzheimer patients (Birge andMortel, 1997; Henderson, 1997). O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
There are a number of points about results of the present study that should be
noted. First, the placebo group was better in the verbal memory test at baseline andstayed better through the experiment. These baseline differences can not beexplained by demographic differences between the two groups and should beconsidered as by chance. However, since our main finding is an association betweentreatment induced estradiol levels and verbal memory changes within the treatmentgroup, these baseline differences do not compromise our data.
Second, the 2 week transdermal estradiol treatment resulted in mean estradiol
levels that are normally observed in the early follicular phase (Mishell et al., 1971),and these values were lower than reference values provided by the manufacturer ofthe patches. Of note is, that subjects from the low treatment induced estradiol levelsgroup, had already lower estradiol levels at baseline, which might suggest, thatthese subjects had a higher estradiol metabolism. Although estradiol levels in thisgroup almost tripled in response to the treatment, the levels were still in thepostmenopausal range. In addition, improper application and/or exchange of thepatch or a difference in estradiol absorbtion by the skin might have contributed tothe low estradiol levels obtained in this group. In contrast, the levels reached by thehigh estradiol increase group were in the lower physiological range of youngwomen. An oral preparation might have lead to a more uniform estradiol increase,which in turn might have lead to different results as obtained in the present study.
Third, when the placebo and the estradiol groups were compared, no treatment
effects could be detected for the cognitive tests or for mood, until these measureswere related to blood estradiol levels. Median split analysis of the treatment grouprevealed that subjects with higher post treatment estradiol levels performed better inthe verbal memory test than subjects with a lower estradiol increase. This result isnot likely to be a statistical artifact, since correlation analysis also revealed anassociation between post treatment estradiol levels and changes in verbal memory. The present study emphasizes the importance of monitoring treatment-inducedestradiol increases in order to be able to relate them to changes in memoryperformance. Several previous epidemiological and experimental studies in this areahave failed to do so (e.g. Caldwell and Watson, 1952; Rauramo et al., 1975; Ditkoffet al., 1991; Barrett-Connor and Kritz-Silverstein, 1993; Robinson et al., 1994;Kimura, 1995; Jacobs et al., 1998).
Our data support the hypothesis that estradiol selectively enhances verbal mem-
ory performance as was previously reported in studies in younger women who hadlow estradiol levels due to surgical or pharmacological treatment (Phillips andSherwin, 1992; Sherwin and Tulandi, 1996). The finding that only delayed, recallwas significantly enhanced suggests that hippocampal mediated changes mightunderlying the observed effects (Eichenbaum et al., 1992; Squire, 1992). Thespecificity of the effects for verbal memory, as opposed to spatial memory, isremarkable, and the underlying mechanisms await to be determined.
The observation that effects on verbal memory can already be detected after 2
weeks is consistent with data obtained in rodents, showing that estradiol fluctuationhas rapid effects on dendritic spines in the hippocampus and on the cholinergicsystem in the forebrain (McEwen and Alves, in press; McEwen et al., 1995, 1997). O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
Such rapid effects on cognition, for example, are not obvious after a 2 weekreplacement with the sex hormone precursor, dehydroepiandrosterone (Wolf et al.,1997, 1998). One line of future research would be to shorten the treatment periodwith estradiol even further to see how rapidly the cognitive effects appear.
Although estradiol treatment also affected mood, this effect was unrelated to
changes in memory performance. This is again in line with previous findingssuggesting that estradiol treatment might modulate mood and cognition via differ-ent pathways as suggested by Sherwin (1997) and also indicated by the diverseneurochemical systems affected by estrogens (McEwen and Alves, in press;McEwen et al., 1995, 1997).
In conclusion, the present data provide preliminary evidence that estradiol
treatment resulting in low physiological levels can elicit significant effects on verbalmemory after a relatively short interval, 2 weeks, in women who were post-menopausal on the average for more than a decade. This suggests that, the braindoes not lose its ability to respond to estradiol even if estradiol levels had been lowfor more than ten years before treatment. Acknowledgements
This study was supported by grants from the Deutsche Forschungsgemeinschaft:
References
Barrett-Connor, E., Kritz-Silverstein, D., 1993. Estrogen replacement therapy and cognitive function in
older women. J. Am. Med. Assoc. 269, 2637 – 2641.
Baeumler, G., 1974. Lern-und Gedaechtnistes (LGT-3): Handanweisung. Hogrefe, Goettingen,
Birge, S.J., Mortel, K.F., 1997. Estrogen and the treatment of Alzheimer’s disease. Am. J. Med. 103,
Caldwell, B.M., Watson, R.I., 1952. An evaluation of psychological effects of sex hormone administra-
tion administration in aged women. I. Results of therapy after six months. J. Gerontol. 7, 228 – 244.
Carlson, L.E., Sherwin, B.B., 1998. Steroid hormones, memory and mood in a healthy elderly
population. Psychoneuroendocrinology 23, 583 – 603.
Convit, A., De Leon, M.J., Tarshish, C., De Santi, S., Tsui, W., Rusinek, H., George, A., 1997. Specific
hippocampal volume reductions in individuals at risk for Alzheimer’s disease. Neurobiol. Aging 18,131 – 138.
Ditkoff, E.C., Crary, W.G., Cristo, M., Lobo, R.A., 1991. Estrogen improves psychological function in
asymptomatic postmenopausal women. Obstet. Gynecol. 78, 991 – 995.
Eichenbaum, H., Otto, T., Cohen, N.J., 1992. The hippocampus — what does it do? Behav. Neural. Biol.
Fedor-Freybergh, P., 1977. The influence of oestrogens on the wellbeing and mental performance in
climacteric and postmenopausal women. Acta Obstet. Gynecol. Scand. 64, 1 – 69.
Gazzaley, A.H., Weiland, N.G., McEwen, B.S., Morrison, J.H., 1996. Differential regulation of
NMDAR1 mRNA and protein by estradiol in the rat hippocampus. J. Neurosci. 16, 6830 – 6838. O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
Gibbs, R.B., Del Rio, G., Velardo, A., et al., 1994. Estrogen and nerve growth factor-related systems in
brain. Effects on basal forebrain cholinergic neurons and implications for learning and memoryprocesses and aging. Ann. NY Acad. Sci. 743, 165 – 196.
Gould, E., Woolley, C.S., Frankfurt, M., McEwen, B.S., 1990. Gonadal steroids regulate dendritic spine
density in hippocampal pyramidal cells in adulthood. J. Neurosci. 10, 1286 – 1291.
Haskell, S.G., Richardson, E.D., Horwitz, R.I., 1997. The effect of estrogen replacement therapy on
cognitive function in women: a critical review of the literature. J. Clin. Epidemiol. 50, 1249 – 1264.
Henderson, V.W., 1997. Estrogen, cognition, and a woman’s risk of Alzheimer’s disease. Am. J. Med.
Horn, W., 1983. Leistungspruefsystem (LPS). Hogrefe, Goettingen, Germany. Jacobs, D.M., Tang, M.X., Stern, Y., et al., 1998. Cognitive function in nondemented older women who
took estrogen after menopause. Neurology 50, 368 – 373.
Kampen, D.L., Sherwin, B.B., 1994. Estrogen use and verbal memory in healthy postmenopausal
women. Obstet. Gynecol. 83, 979 – 983.
Kimura, D., 1995. Estrogen replacement therapy may protect against intellectual decline in post-
menopausal women. Horm. Behav. 29, 312 – 321.
Luine, V.N., Khylchevskaya, R.I., McEwen, B.S., 1975. Effect of gonadal steroids on activities of
monoamine oxidase and choline acetylase in rat brain. Brain Res. 86, 293 – 306.
McEwen, B.S., Alves, S.E., Bulloch, K., Weiland, N.G., 1997. Ovarian steroids and the brain:
implications for cognition and aging. Neurology 48, S8 – 15.
McEwen, B.S., Gould, E., Orchinik, M., Weiland, N.G., Woolley, C.S., 1995. Oestrogens and the
structural and functional plasticity of neurons: implications for memory, ageing and neurodegenera-tive processes. Ciba Found. Symp. 191, 52 – 66.
McEwen, B.S., Alves, S. Estrogen action in the central nervous system. Endocr Rev (in press)Mishell, D.R., Nakamura, R.M., Stone, S., Khamara, K., Nagata, Y., Thorneycroft, L.H., 1971. Serum
gonadotropin and steroid patterns during the normal menstrual cycle. Gynecology 11, 60 – 65.
Oswald, W.D., Fleischmann, U.M., 1994. Nuernberger Alters Inventar (NAI). Hogrefe, Goettingen,
Owen, A.M., 1997. The functional organization of working memory processes within human lateral
frontal cortex: the contribution of functional neuroimaging. Eur. J. Neurosci. 9, 1329 – 1339.
Phillips, S.M., Sherwin, B.B., 1992. Effects of estrogen on memory function in surgically menopausal
women. Psychoneuroendocrinology 17, 485 – 495.
Polo-Kantola, P., Portin, R., Polo, O., Helenius, H., Irjala, K., Erkkola, R., 1998. The effect of
short-term estrogen replacement therapy on cognition: a randomized, double-blind, cross-over trialin postmenopausal women. Obstet. Gynecol. 91, 459 – 466.
Rauramo, L., Lagerspetz, K., Engblom, P., Punnonen, R., 1975. The effect of castration and peroral
estrogen therapy on some psychological functions. Front. Horm. Res. 3, 94 – 104.
Rice, M.S., Graves, A.B., McCurry, S.M., Larson, E.B., 1997. Estrogen replacement therapy and
cogntive function in postmenopausal women without dementia. Am. J. Med. 103, S26 – S35.
Robinson, D., Friedman, L., Marcus, R., Tinklenberg, J., Yesavage, J., 1994. Estrogen replacement
therapy and memory in older women. J. Am. Geriatr. Soc. 42, 919 – 922.
Sarter, M., Bruno, J.P., 1997. Cognitive functions of cortical acetylcholine: toward a unifying hypothe-
sis. Brain. Res. Rev. 23, 28 – 46.
Sherwin, B.B., 1988. Estrogen and/or androgen replacement therapy and cognitive functioning in
surgically menopausal women. Psychoneuroendocrinology 13, 345 – 357.
Sherwin, B.B., 1997. Estrogen effects on cognition in menopausal women. Neurology 48, S21 – S26. Sherwin, B.B., Tulandi, T., 1996. ‘Add-back’ estrogen reverses cognitive deficits induced by a go-
nadotropin-releasing hormone agonist in women with leiomyomata uteri. J. Clin. Endocrinol. Metab. 81, 2545 – 2549.
Singh, M., Meyer, E.M., Simpkins, J.W., 1995. The effect of ovariectomy and estradiol replacement on
brain-derived neurotrophic factor messenger ribonucleic acid expression in cortical and hippocampalbrain regions of female Sprague – Dawley rats. Endocrinology 136, 2320 – 2324.
Squire, L.R., 1992. Memory and the hippocampus: a synthesis from findings with rats, monkeys, and
humans. Psychol. Rev. 99, 195 – 231. O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
Steyer, R., Schwenkmezger, P., Notz, P., Eid, M., 1994. Testtheoretische analysen des mehrdimen-
sionalen befindlichkeitsfragebogens (MDBF). Diagnostica 40, 320 – 328.
Stroop, J.R., 1935. Studies of interference in serial verbal reactions. J. Exp. Psych. 18, 643 – 662. West, R.L., 1996. An application of prefrontal cortex function theory to cognitive aging. Psychol. Bull.
Wolf, O.T., Naumann, E., Hellhammer, D.H., Kirschbaum, C., 1998. Effects of deyhdroepiandrosterone
(DHEA) replacement in elderly men on event related potentials (ERPs), memory and well-being. J. Gerontol. 53, M385 – 390.
Wolf, O.T., Neumann, O., Hellhammer, D.H., et al., 1997. Effects of a two-week physiological
dehydroepiandrosterone substitution on cognitive performance and well-being in healthy elderlywomen and men. J. Clin. Endocrinol. Metab. 82, 2363 – 2367.
Woolley, C.S., McEwen, B.S., 1992. Estradiol mediates fluctuation in hippocampal synapse density
during the estrous cycle in the adult rat. J. Neurosci. 12, 2549 – 2554.
Woolley, C.S., McEwen, B.S., 1994. Estradiol regulates hippocampal dendritic spine density via an
N-methyl-D-aspartate receptor-dependent mechanism. J. Neurosci. 14, 7680 – 7687.
Woolley, C.S., Weiland, N.G., McEwen, B.S., Schwartzkroin, P.A., 1997. Estradiol increases the
sensitivity of hippocampal CA1 pyramidal cells to NMDA receptor-mediated synaptic input:correlation with dendritic spine density. J. Neurosci. 17, 1848 – 1859.
Origami, Eleusis, and the Soma Cube: Martin Gardner's Mathematical Diversions, , Martin Gardner,Cambridge University Press, 2008, 0521735246, 9780521735247, 234 pages. Martin Gardner continues todelight readers in Origami, Eleusis, and the Soma Cube, which is the second volume in the new Cambridgeseries, The New Martin Gardner Mathematical Library, based off his enormously popular Scientific Ame
ESM (REscuers checklist)1. Scene assessment i. Check the environment ii. Check the peopleiii. Check the Mechanism of Injury (MOI)iv. Assure your own safety (Gloves)b. Control the scene (Assert your authority as a first aider)c. Introduce yourself and get Consent A - This is established if the patient is talking to you B - Ask the patient to take a breath. Note any abnormalities C - Ask

 Psychoneuroendocrinology 24 (1999) 727 – 741
Two weeks of transdermal estradiol treatment
in postmenopausal elderly women and its effect
on memory and mood: verbal memory changes
are associated with the treatment induced
Oliver T. Wolf a,b,c, Brigitte M. Kudielka a,
Dirk H. Hellhammer a, Sonja To¨rber a, Bruce S. McEwen b,
a Center for Psychobiological and Psychosomatic Research, Uni6ersity of Trier, Dietrichstraße 10-11,
b Laboratory of Neuroendocrinology, Rockefeller Uni6ersity, New York, NY, USA
c Neuroimaging Laboratory, Department of Psychiatry, NYU School of Medicine, New York, NY, USA
Received 18 December 1998; accepted 12 April 1999
Abstract
Psychoneuroendocrinology 24 (1999) 727 – 741
Two weeks of transdermal estradiol treatment
in postmenopausal elderly women and its effect
on memory and mood: verbal memory changes
are associated with the treatment induced
Oliver T. Wolf a,b,c, Brigitte M. Kudielka a,
Dirk H. Hellhammer a, Sonja To¨rber a, Bruce S. McEwen b,
a Center for Psychobiological and Psychosomatic Research, Uni6ersity of Trier, Dietrichstraße 10-11,
b Laboratory of Neuroendocrinology, Rockefeller Uni6ersity, New York, NY, USA
c Neuroimaging Laboratory, Department of Psychiatry, NYU School of Medicine, New York, NY, USA
Received 18 December 1998; accepted 12 April 1999
Abstract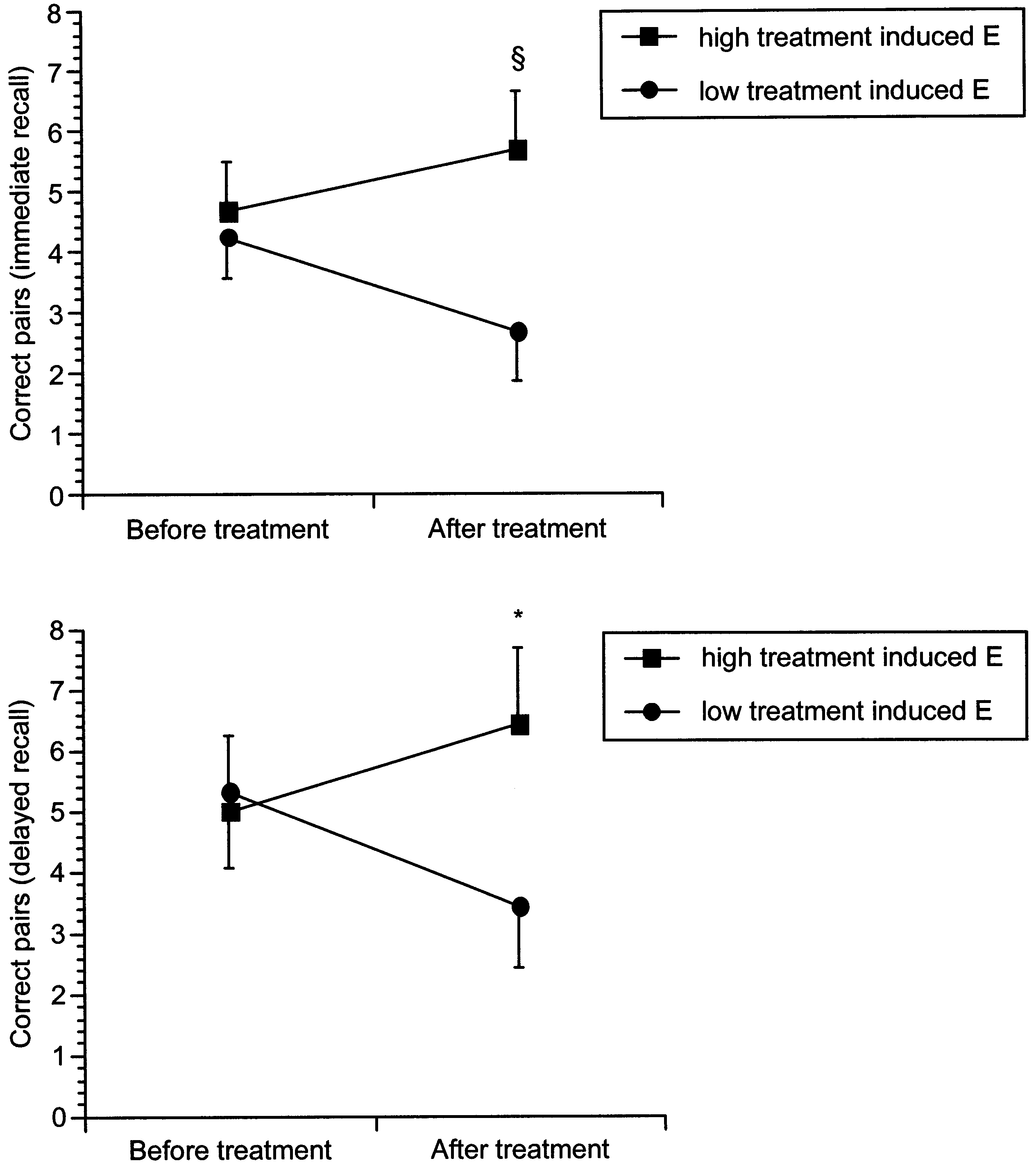 O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
Fig. 1. Immediate (top) and delayed (bottom) verbal memory performance in women with high versuslow treatment induced estradiol levels in response to the 2 week transdermal estradiol treatment;* P B05 and § PB0.10 in post hoc comparison. The estradiol levels of the two groups are presented inTable 3.
O.T. Wolf et al. / Psychoneuroendocrinology 24 (1999) 727 – 741
Fig. 1. Immediate (top) and delayed (bottom) verbal memory performance in women with high versuslow treatment induced estradiol levels in response to the 2 week transdermal estradiol treatment;* P B05 and § PB0.10 in post hoc comparison. The estradiol levels of the two groups are presented inTable 3.