Tadalafil zeigt eine konstante Resorption im Gastrointestinaltrakt, mit maximalen Plasmaspiegeln nach rund zwei Stunden. Der Wirkstoff verteilt sich gut im Gewebe und weist eine hohe Plasmaproteinbindung auf. Seine lange Halbwertszeit erlaubt eine verlängerte Wirkphase. Der Metabolismus erfolgt über das hepatische Enzymsystem CYP3A4, mit der Bildung inaktiver Metaboliten. Exkretion geschieht primär über den Stuhl. Die Häufigkeit von Nebenwirkungen steigt mit der Dosis, wobei vor allem vasodilatatorische Effekte dominieren. Ein gängiger Bezugspunkt in pharmakologischen Analysen ist cialis ohne rezept, das mit dieser Wirkstoffklasse assoziiert ist.
Ejd;01jun99
Psychopharmacology (1999) 143 : 286 –292
P. Bitsios · E. Szabadi · C.M. Bradshaw
Comparison of the effects of venlafaxine, paroxetine and desipramineon the pupillary light reflex in man
Received : 29 July 1998 / Final version : 17 November 1998
Abstract Rationale : The time-course of the pupillary
effects. Conclusions : The increase in resting pupil diam-
light reflex response is determined by the successive
eter could be indicative of parasympathetic inhibition
activation of the parasympathetic and sympathetic
and / or sympathetic activation. The shortening of the
innervations of the iris, the latency and the amplitude
recovery time of the light reflex response is consistent
reflecting parasympathetic and the recovery time
with sympathetic potentiation resulting from nora-
mainly sympathetic activity. Objective : To compare the
drenaline uptake blockade in the iris. The prolonga-
effects of single doses of three antidepressants (ven-
tion of the latency and decrease of the amplitude of
lafaxine : serotonin / noradrenaline reuptake inhibitor,
the light reflex response are indicative of a parasym-
paroxetine : selective serotonin reuptake inhibitor, and
patholytic effect of venlafaxine. However, as venlafax-
desipramine : tricyclic antidepressant) on resting pupil
ine has negligible affinity for muscarinic cholinoceptors,
diameter and the pupillary light reflex response.
this effect cannot be attributed to the blockade of
Methods : Fifteen healthy male volunteers participated
cholinoceptors in the iris. A possible explanation for
in five weekly sessions, each of which was associated
this finding is that it reflects a central rather than a
with one treatment (venlafaxine 75 mg or 150 mg,
peripheral effect of the drug : the blockade of nora-
paroxetine 20 mg, desipramine 100 mg, or placebo)
drenaline uptake in the brain could lead to the poten-
according to a double-blind, double-dummy, balanced,
tiation of the noradrenergic inhibition of central
cross-over design. An infrared binocular television
parasympathetic (Edinger-Westphal) neurones. These
pupillometer was used for the recording of the resting
results demonstrate the ability of therapeutically rele-
pupil diameter and the pupillary light reflex in dark-
vant single doses of venlafaxine to potentiate nora-
ness, in previously dark-adapted eyes. Resting pupil
drenergic responses in man, consistent with the
diameter in darkness was recorded before and after
treatment. The pupillary light reflex was elicited aftertreatment, with six light flashes (green, 565 nm peak
Key words Light reflex · Pupil · Venlafaxine ·
wavelength) of 200 ms duration and of incremental
Paroxetine · Desipramine · Human volunteers
illuminance (measured in the plane of the cornea) :3.0 × 10–3, 8.5 × 10–3, 2.5 × 10–2, 7.0 × 10–2, 0.18,0.43 mW cm92. The parameters studied were : latency,amplitude and 75 % recovery time. Results : Analyses
of variance followed by post hoc tests (least significantdifference test or Dunnett’s test; P < 0.05) revealed that
Venlafaxine is an antidepressant with serotonin and
both doses of venlafaxine produced a significant
noradrenaline uptake inhibiting properties (SNRI)
increase in resting pupil diameter, decrease in ampli-
with a weak effect on dopamine uptake (Muth et al.
tude and shortening of the 75 % recovery time of the
1986; Bolden-Watson and Richelson 1993). Venla-
light reflex response; venlafaxine 150 mg prolonged the
faxine does not inhibit monoamine oxidase A or B
latency, while the other treatments had no significant
(Muth et al. 1986) and does not have anticholinergic,antiadrenergic, antiserotonergic or antihistaminergicproperties (Preskorn 1994). It is believed that at
P. Bitsios · E. Szabadi (*) · C.M. Bradshaw
lower doses venlafaxine acts mainly as a serotonin re-
Department of Psychiatry, University of Nottingham,
uptake inhibitor, whereas at higher doses, it exerts an
Floor A, South Block, Queen’s Medical Centre,Nottingham NG7 2UH, UK
additional noradrenergic re-uptake inhibition (Muth
et al. 1986; Richelson 1994). The latter has been
thought to account for venlafaxine’s increased efficacyin severely depressed patients when higher doses are
used (DeMontigny and Preskorn 1995; Preskorn 1995).
There is little evidence, however, that venlafaxine
Fifteen healthy male volunteers aged 20–28 years (mean ± SEM
inhibits noradrenaline re-uptake at clinically used doses
22.00 ± 1.0) and weighing 57–105 kg (mean ± SEM 76.0 ±5.8) par-
in humans, or that noradrenergic uptake blockade
ticipated in the study. Subjects were all medication-free and wererequested to stop smoking and to avoid drinking alcohol, coffee
occurs mainly at the upper limits of the recommended
and other caffeine-containing beverages for at least 12 h before the
dosage range. In a recent single dose study, venlafax-
experimental session. All of them were using tobacco and caffeine
ine 150 mg, but not venlafaxine 75 mg, potentiated the
occasionally and all were occasional social alcohol consumers. They
venoconstrictor response to noradrenaline in healthy
were all tested in the morning hours (9 : 00 a.m.–14 : 00 p.m.). Thestudy protocol was approved by the University of Nottingham
volunteers, consistent with the postulated noradrener-
Medical School Ethics Committee. All volunteers gave their writ-
gic re-uptake inhibiting effect of the drug at higher
ten consent following a verbal explanation of the study and after
dosage levels (Abdelmawla et al. 1997a).
reading a detailed information sheet.
The human pupil is a suitable, non-invasive system
to test noradrenergic responses in humans, in vivo. Mydriasis evoked by systemically administered drugs
may be the result of increased sympathetic or reduced
Venlafaxine 75 mg and 150 mg, paroxetine 20 mg, desipramine
parasympathetic influence on the iris, or both, and
100 mg, and placebo were administered orally in matching capsules.
drug-induced miosis may be the result of decreased
In each session the subjects ingested one capsule on two occasions :
sympathetic or increased parasympathetic influence
one of the capsules contained the active drug and the other the
on the iris, or both. The pupillary light reflex response
placebo, except in the placebo session when both capsules containedplacebo. The first capsule, containing desipramine, paroxetine or
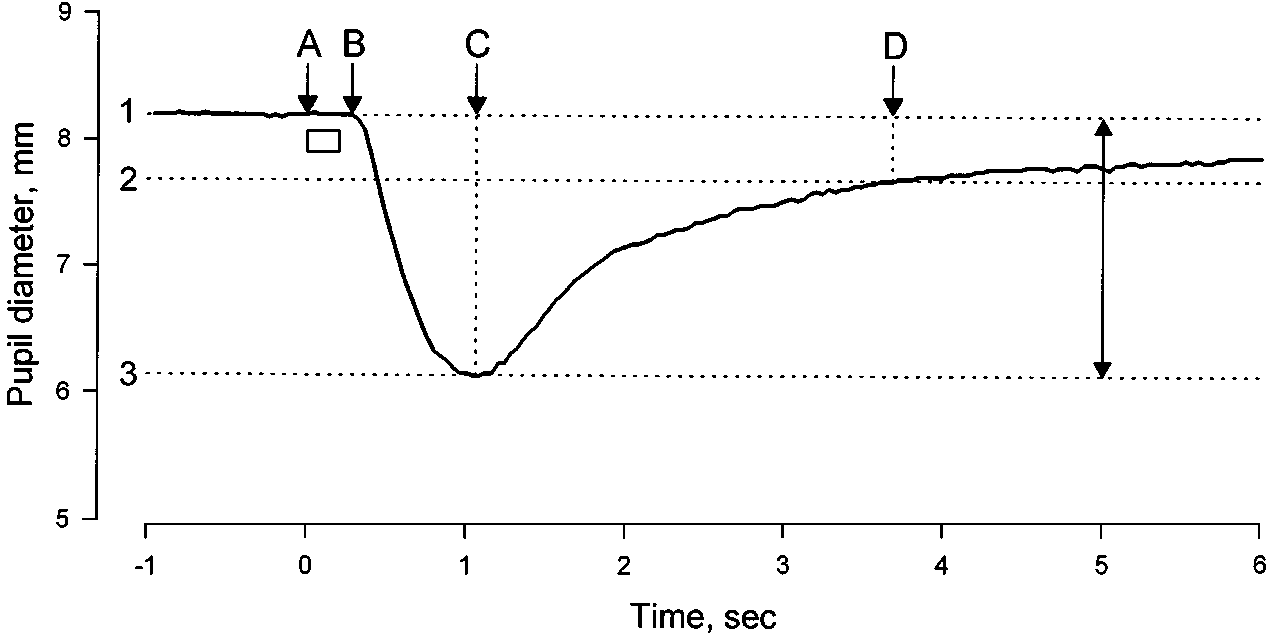
(see Fig. 1.) may help to elucidate the effects of a drug
placebo was ingested 180 min and the second capsule, containing
on the sympathetic and parasympathetic inputs to venlafaxine 75 mg, venlafaxine 150 mg or placebo, 100 min priorthe iris, since the time-course of the light reflex response
is determined by the successive activation of theparasympathetic and sympathetic inputs, latency andamplitude reflecting parasympathetic activation, and
recovery time reflecting mainly sympathetic activation(Loewenfeld 1993).
Subjects participated in five weekly sessions. Subjects were allocated
The aim of this study was to provide evidence for
to drugs and sessions according to a double-blind, balanced, cross-
the noradrenaline re-uptake inhibiting property of ven-
over design. A double-dummy procedure (see above, Drugs) was
lafaxine in healthy volunteers using the pupillary light
adopted in order to account for the different absorption kinetics ofthe active drugs. It has been reported that the peak concentration
reflex as a test system. We used desipramine, a tricyclic
after a single oral dose of desipramine (Sallee and Pollock 1990)
antidepressant with potent noradrenaline re-uptake
and paroxetine (Kaye et al. 1990) is attained approximately 3 h after
inhibiting properties but little action on serotonin re-
ingestion, whereas the peak concentration is obtained approxi-
uptake (Richelson 1994), and paroxetine, a selective
mately 2 h after the ingestion of venlafaxine (Kamerus et al. 1992).
serotonin re-uptake inhibitor with little effect on nora-drenaline re-uptake (Richelson and Nelson 1984), as
controls. Some of these results have been communi-cated to the British Association for Psychopharma-
An infrared binocular television pupillometer (TVP 1015B Applied
Science Laboratories, Waltham, Mass., USA) was used for the
Fig. 1 Example of a light reflex response. Ordinate : pupil diameter (mm), abscissa : running time (s). Horizontal bar : light stimulus; 1 initial pupil diameter; 2 75 % recovery; 3 pupil diameter at maximal constriction; A onset of light stimulus; B onset of response; C time of maximal constriction; D time at which 75 % recovery is attained; 1–3 amplitude; AB latency; CD 75 % recovery time
recording of resting pupil diameter and the pupillary light reflex indarkness, in previously dark-adapted eyes. The experimental ses-sion started with three 45-s recordings of resting pupil diameter,the average of which served as the pre-treatment baseline restingpupil diameter. Three hours after ingestion of the first capsule(100 min after ingestion of the second capsule), recordings of rest-ing pupil diameter were repeated and then the pupillary light reflexresponse was studied. The stimuli were six light flashes (green,565 nm peak wavelength) of 200 ms duration, and of incrementalilluminance (measured in the plane of the cornea) : 3.0 × 1093, 8.5 × 1093, 2.5 × 1092, 7.0 × 1092, 0.18, 0.43 mW cm91. The lightflashes were delivered at 25 s intervals, via a light emitting diodepositioned 1 cm from the cornea of the subject’s right eye. Therecordings took place in a dark, sound-attenuated room and thesubjects fixed their gaze on a dim red spot of light positioned approx-imately 2.5 m in front of them. Stimulus presentation was controlledby a microcomputer, and pupillary measures were digitized andstored on a floppy disk for off-line analysis. The parameters stud-ied were : latency (i.e. time elapsing from the onset of the stimulusto the onset of the response, s), amplitude of light reflex response(i.e. the difference between the initial and the minimal diameters ofa pupillary response to a light flash, mm) and 75 % recovery time(i.e. time taken from the peak of the response to obtain 75 % recov-ery, s) (see Fig. 1). Each light reflex response was visually inspected. If an eye-blink occurred either during the presentation of the stim-ulus, reducing the amount of light reaching the retina, or at thepeak of pupillary constriction, rendering the amplitude immea-sureable, the response in question was not included in the analysis. Fig. 2 Change in resting pupil diameter in darkness (mm) from pre- treatment baseline, in the presence of the five treatments. P : placebo, Px 20 : paroxetine 20 mg, V75 : venlafaxine 75 mg, V150 : venlafaxine 150 mg, DMI100 : desipramine 100 mg. The heights of
the columns correspond to the means obtained in the group of 15subjects; vertical bars are SEM. Asterisks denote statistical
Data obtained from the left pupil were analyzed. The post / pre-
treatment difference was calculated for resting pupil diameter indarkness for each subject and for the group of 15 subjects. One-way analysis of variance with repeated measures with treatment as
Table 1 Effects of treatments on pupil diameter (mm) : differences
the within-subject factor followed by post hoc tests (least significant
difference test) were used to compare the effects of treatment onresting pupil diameter in darkness. Separate two-way analyses of
variance with repeated measures, with treatment (five levels) and
light intensity (six levels) as the within-subject factors, were used toanalyze each light reflex measure (i.e. latency, amplitude, 75 % recov-
ery time). In the case of a significant effect of treatment, multiple
comparisons between placebo and the four active treatments were
undertaken using Dunnett’s test (df = 56, k = 5, criterion P < 0.05).
The relationship between response amplitude and recovery time wasanalyzed using the product moment correlation coefficient, and bestfit linear functions were derived with the method of least squares.
lafaxine 75 mg and more so with venlafaxine 150 mg.
Unpaired t-test was used to compare the slope values for each active
Analysis of variance of the latency data revealed
significant main effects of treatment (F = 5.19; df: 4,56,P < 0.001) and light intensity (F = 83.5; df: 5,70;P < 0.001) but no significant interaction (F < 1).
Comparisons between placebo and the four active treat-ments using Dunnett’s test showed that only the effect
The effects of the treatments on resting pupil diameter
of venlafaxine 150 mg was significant (t = 3.70).
in darkness are shown in Fig. 2 and Table 1. It can be
It can be seen that amplitude was smaller with ven-
seen that all treatments caused an increase in resting
lafaxine 75 mg than under the placebo condition, and
pupil diameter. One-way analysis of variance showed
more so with venlafaxine 150 mg. Analysis of variance
that the effect of treatment was significant (F = 4.2;
of the amplitude data revealed significant main effects
df: 4,56; P < 0.005). Post hoc comparisons with the
of treatment (F = 21.8; df: 4,56; P < 0.001) and light
least significant difference test showed that only the
intensity (F = 339.6; df: 5,70; P < 0.001) but no
increases caused by 75 and 150 mg of venlafaxine were
significant interaction (F = 1; df: 20,280; P > 0.1).
Comparisons between placebo and the four active treat-
The latency, amplitude and 75 % recovery time of the
ments using Dunnett’s test showed that the effects of
light reflex response (group means) are displayed in Fig.
venlafaxine 75 and 150 mg were significant (t = 5.46
3. It can be seen that latency was prolonged with ven-
Fig. 3 Parameters of the light reflex response obtained at six graded illuminance levels, measured in the plane of the cornea, in the presence of the five treatments. Open circles : placebo; open triangles : paroxetine; open squares : desipramine; closed triangles : venlafaxine 75 mg; closed squares : venlafaxine 150 mg
It can be seen that recovery time was shorter with
both venlafaxine treatments. Analysis of variance ofthe recovery time data revealed significant main effectsof treatment (F = 4.84; df: 4,56; P < 0.002) and lightintensity (F = 24.9; df: 5,70; P < 0.001) but nosignificant interaction (F < 1). Comparisons betweenplacebo and the four active treatments using Dunnett’stest showed that the effects of venlafaxine 75 and150 mg were significant (t = 2.79 and 3.45, respec-tively).
The possibility that the changes in light reflex recov-
ery time were secondary to changes in amplitude wasalso explored. The relationship between reflex responseamplitude and 75 % recovery time, at each light inten-sity value studied, is shown in Fig. 4; the results of thelinear regression analysis are displayed in Table 2. Itcan be seen from Fig. 4 that the regression linesobtained after placebo and paroxetine did not deviatefrom each other, whereas the regression lines obtainedafter desipramine and venlafaxine deviated from thatobtained after placebo. Statistical comparison of theslopes of the regression lines obtained in the presence
Fig. 4 Relationship between the amplitude and 75 % recovery time
of the antidepressants and placebo showed that the
of the light reflex responses evoked by the range of light stimulus
slopes obtained after the two doses of venlafaxine
intensities shown in Fig. 3. Open circles : placebo; closed circles :
significantly differed from that obtained after placebo
active treatment; the dotted lines were fitted with linear regression
(unpaired t-test : venlafaxine 75 mg versus placebo
analysis; for statistical analysis see text and Table 1
t = 3.09, df: 10, P < 0.02; venlafaxine 150 mg versusplacebo t = 3.71, df: 10, P < 0.01). There were no sta-
size (Loewenfeld 1993). Tricyclic antidepressants have
tistically significant differences between the slopes
variable effects on resting pupil diameter, depending on
obtained after paroxetine and placebo (t = 0.34, df: 10,
the balance between their ability to block noradrena-
P > 0.1) or desipramine and placebo (t = 0.86, df: 10,
line uptake / post-junctional muscarinic cholinoceptors,
effects which would tend to increase pupil diameter,and their ability to block post-junctional α1-adreno-ceptors, an effect which would tend to decrease pupil
diameter (Szabadi and Bradshaw 1986). The tricyclicantidepressant used in the present experiment,
Resting pupil diameter reflects the balance between the
desipramine, is a potent inhibitor of noradrenaline
opposing sympathetic and parasympathetic innerva-
reuptake and has relatively low affinities for muscarinic
tions of the iris, sympathetic activation increasing and
cholinoceptors and α1-adrenoceptors (Richelson
parasympathetic activation decreasing resting pupil
1994). The predicted effect of desipramine on resting
Table 2 Results of linear
regression analysis (leastsquares, product moment
*Slope significantly different from placebo condition, P < 0.02 (see text)
pupil size would be mydriasis, reflecting mainly nora-
mydriasis caused by venlafaxine was due to the block-
drenaline reuptake. In the present experiment, a single
ade of 5HT (re)uptake. Furthermore, the selective nora-
dose (100 mg) of desipramine failed to have a
drenaline reuptake inhibitor (NARI) reboxetine, which
significant effect on pupil diameter, consistent with a
has virtually no affinity for 5HT uptake (Brunello and
previous observation in our laboratory (Theofilopoulos
Racagni 1998), also causes mydriasis (Szabadi et al.
et al. 1995). It should be noted, however, that in some
1998), supporting the hypothesis that the mydriatric
other studies a mydriatic effect of desipramine could
effect of venlafaxine is due to the blockade of nora-
be observed (Szabadi et al. 1980, 1998; Shur and
Checkley 1982; Kerr and Szabadi 1985). It seems, there-
It is well known that there is a correlation between
fore, that the mydriasis observed after the administra-
the level of physiological arousal and pupil diameter,
tion of desipramine is not a consistent finding. The
sedation being accompanied by miosis and activation
basis for the inconsistency may lie in the fact that
by mydriasis (Loewenfeld 1993). In this respect, it is of
desipramine also blocks α1-adrenoceptors, and the rela-
interest that venlafaxine has been reported to have a
tionship between the mydriasis resulting from nora-
desipramine-like activating effect on the EEG, espe-
drenaline reuptake blockade and the miosis from
cially at a dosage of 50 mg and above (Saletu et al.
α1-adrenoceptor blockade may differ between different 1992; Patat et al. 1998). Furthermore, venlafaxineexperiments.
shows some alerting effect in both psychophysiological
Both single doses (75 and 150 mg) of venlafaxine
tests (e.g. critical flicker fusion frequency) and subjec-
caused an increase in dark-adapted resting pupil diam-
tive ratings of level of alertness (Saletu et al. 1998). It
eter. This observation is in agreement with an earlier
is likely that the alerting effect of venlafaxine is due to
report demonstrating the mydriatic effect of smaller sin-
central noradrenergic activation (Foote and Aston-
gle doses (12.5, 25 and 50 mg) of venlafaxine (Saletu
Jones 1995) resulting from the blockade of noradren-
et al. 1992). As venlafaxine has practically no affinity
aline uptake in the brain. Interestingly, central
for muscarinic cholinoceptors (Preskorn 1994), but has
noradrenergic activation may also contribute to the
the ability to block noradrenaline uptake (Muth et al.
mydriasis by enhancing the tonic noradrenergic inhi-
1986; Richelson 1994), the most likely explanation for
bition of the Edinger-Westphal nucleus (see below).
venlafaxine-evoked mydriasis is that it reflects the
Venlafaxine also had distinctive effects on the kinetic
blockade of noradrenaline uptake into sympathetic
parameters of the light reflex response, prolonging
nerve terminals in the iris, which in turn results in the
the latency, reducing the amplitude and shortening
potentiation of the influence of the sympathetic input
the recovery time of the response. The shortening of the
recovery time could have been secondary to the reduc-
As venlafaxine blocks not only noradrenaline but
tion in the amplitude of the reflex response, since it is
also 5-hydroxytryptamine (re)uptake in the brain
well documented that smaller light reflex responses take
(Muth et al. 1986; Richelson 1994), it should be con-
a shorter time to recover (Smith 1988; Theofilopoulos
sidered whether the mydriasis evoked by venlafaxine
et al. 1995). However, it is unlikely that the reduction
might have been, at least partly, mediated by a sero-
in amplitude can fully explain the shortening of the
tonergic mechanism. Indeed, there is evidence that such
recovery time in the present experiment, since the sta-
mechanisms may be involved in pupillary control. Thus
tistical analysis of the relationship between amplitude
it has been reported that both 5-HT2 receptor antag-
and recovery time showed that the two doses of ven-
onists (Millson et al. 1991, 1992) and 5HT1A receptor
lafaxine shortened the recovery time over and above
agonists (Fanciullacci et al. 1995; Phillips et al. 1998)
that predicted on the basis of a reduction in amplitude
cause miosis. On the other hand, fenfluramine, a drug
alone. Thus, the shortening of the recovery time seems
known to release 5HT from pre-synaptic terminals,
to be consistent with a genuine alteration in the auto-
increases pupil diameter (Kramer et al. 1973). However,
nomic components of the light reflex response. In fact,
therapeutically relevant single doses of the SSRIs
the effect on the recovery time is consistent with the
fluvoxamine (50–100 mg : Wilson et al. 1983; Flett
blockade of noradrenaline uptake in the iris, leading
et al. 1992) and paroxetine (20 mg : present study),
to sympathetic potentiation. There is evidence that the
when compared to placebo, have no significant effect
recovery time is modulated by sympathetic activity :
on pupil diameter. Therefore, it is unlikely that the
variables which increase sympathetic activity [e.g. heat
stressor (Leung et al. 1992; Mortlock et al. 1996)]
prolongation of the latency and reduction of the ampli-
shorten the recovery time, whereas variables which
tude of the light reflex response, and, to some extent,
decrease the sympathetic influence on the iris [e.g. the
the mydriasis). It is of interest that venlafaxine, like the
centrally acting sympatholytic drug clonidine (Morley
selective noradrenaline reuptake inhibitor reboxetine
et al. 1991) and the α1-adrenoceptor antagonist pra-
(Szabadi et al. 1998), displays a similar pseudo-
zosin (Mortlock et al. 1996)] prolong the recovery time.
anticholinergic effect on salivary gland activity
Again, this effect was not shared by the SSRI paroxe-
(Abdelmawla et al. 1997b), probably resulting from the
tine, consistent with previous findings with another
potentiation of the central noradrenergic inhibition of
SSRI, fluvoxamine (Flett et al. 1992), indicating that
the salivary nuclei in the brain stem.
central 5HT reuptake blockade by venlafaxine is
In the present study, both single doses (75 and
unlikely to be involved in the shortening of the recov-
150 mg) of venlafaxine exerted effects consistent with
ery time. Furthermore, the selective noradrenaline
the blockade of noradrenaline uptake both in the
reuptake inhibitor reboxetine, which has no effect on
periphery and the central nervous system. It is of inter-
5HT uptake, causes a similar shortening of the recov-
est that in another report (Abdelmawla et al. 1997a),
ery time of the light reflex response (Theofilopoulos et
in which the effects of the same doses of venlafaxine
on noradrenergic responses of the dorsal hand vein
The prolongation of the latency and reduction of
were studied, only the higher dose potentiated the
amplitude of the light reflex response, observed after
response to noradrenaline. These observations indicate
the administration of venlafaxine, are surprising
a difference between the effects of the drug on responses
findings, since these effects are generally attributed to
evoked by endogenously released and exogenously
parasympathetic inhibition (Smith 1988), and ven-
applied noradrenaline : for potentiation of responses to
lafaxine has virtually no affinity for muscarinic
exogenously applied noradrenaline higher dosages of
cholinoceptors (Preskorn 1994). An alternative expla-
venlafaxine are required than for the potentiation of
nation may be that this “pseudo-anticholinergic” effect
the effects of endogenously released noradrenaline.
of venlafaxine is due to noradrenergic potentiation in
Therefore, it is likely that patients treated even with
the brain, again resulting from noradrenaline uptake
lower dosages of venlafaxine may experience some
blockade. There is evidence that the pre-ganglionic
enhancement of the pharmacodynamic effects of
parasympathetic cholinergic neurones in the Edinger-
Westphal nucleus of the mid-brain are under tonicinhibitory noradrenergic control from the locus
Acknowledgements We are grateful to Wyeth Laboratories for financial support. P.B. was supported by a scholarship from the
coeruleus (for review, see Szabadi and Bradshaw 1996) :
State Scholarship Foundation of Greece (I.K.Y.).
the blockade of noradrenaline uptake at the inhibitorynoradrenergic synapses in the Edinger-Westphalnucleus would “switch off ” the parasympathetic neu-rones, resulting in a pseudo-anticholinergic effect in the
periphery. Indeed, the opposite effect, i.e. disinhibitionresulting in the enhancement of the light reflex
Abdelmawla A, Langley RW, Szabadi E, Bradshaw CM (1997a)
response, can be observed when the inhibitory input
Comparison of venlafaxine, desipramine and paroxetine on thedorsal hand vein in man. J Psychopharmacol 11 : A28
from the locus coeruleus is “switched off ” by the α2-
Abdelmawla A, Bitsios P, Langley RW, Szabadi E, Bradshaw CM
adrenoceptor agonist clonidine (Szabadi and Bradshaw
(1997b) Comparison of venlafaxine, desipramine and paroxe-
1996). It is of interest that the selective noradrenaline
tine on autonomic functions in man. J Pychopharmacol
reuptake inhibitor reboxetine, which like venlafaxine
Bitsios P, Langley RW, Szabadi E, Bradshaw CM (1997)
has little affinity for muscarinic cholinoceptors
Comparison of venlafaxine, desipramine and paroxetine on the
(Brunello and Racagni 1998), has a similar inhibitory
pupillary light reflex in man. J Psychopharmacol 11 : A28
(“pseudo-anticholinergic”) effect on the light reflex
Bolden-Watson C, Richelson E (1993) Blockade by newly-devel-
response (Theofilopoulos et al. 1995).
oped antidepressants of biogenic amine uptake into rat brain
In conclusion, the pupillary effects of single doses of
Brunello N, Racagni G (1998) Rationale for the development of
venlafaxine are consistent with the ability of the drug
noradrenaline reuptake inhibitors. Hum Psychopharmacol
to block noradrenaline reuptake and thereby potenti-
ate the pharmacological effects of endogenously
DeMontigny E, Preskorn SH (1995) Comparison of the tolerabil-
released noradrenaline. The blockade of noradrenaline
ity of bupropion, fluoxetine, imipramine, nefazadone, paroxe-tine, sertraline, and venlafaxine. J Clin Psychiatry 56 : 2–21
reuptake at the noradrenergic sympathetic effector
Fanciullacci M, Sicuteri R, Alessandri M, Geppetti P (1995)
junction in the iris could explain the mydriasis and the
Buspirone, but not sumatriptan, induces miosis in humans : rel-
shortening of the recovery time of the light reflex
evance for a serotoninergic pupil control. Clin Pharmacol Ther
response, whereas the blockade of noradrenaline reup-
take at the inhibitory noradrenergic synapses on
Flett SR, Szabadi E, Bradshaw CM (1992) A comparison of
the effects of fluvoxamine and amitriptyline on autonomic
Edinger-Westphal neurones may be responsible for the
functions in healthy volunteers. Eur J Clin Pharmacol 42 :
pseudo-anticholinergic pupillary effects of the drug (i.e.
Foote SL, Aston-Jones GS (1995) Pharmacology and physiology
Phillips MA, Szabadi E, Bradshaw CM (1998) Effects of the anxi-
of central noradrenergic systems. In : Bloom FE, Kupfer DJ
olytics lesopitron and buspirone on the human pupil. J
(eds) Psychopharmacology : the fourth generation of progress.
Preskorn SH (1994) Antidepressant drug selection : criteria and
Kaye CM, Haddock PF, Langley G, Mellows TCG, Zussman TBD,
Greb WH (1989) A review of the metabolism of paroxetine in
Preskorn SH (1995) Clinical pharmacology of SSRIs : the basis for
their optimal use. Professional Communication Caddo,
Kerr FA, Szabadi E (1985) Comparison of the effects of chronic
administration of ciclazindol and desipramine on pupillary
Richelson E (1994) Pharmacology of antidepressants; characteris-
responses to tyramine, methoxamine and pilocarpine in healthy
tics of ideal drug. Mayo Clin Proc 69 : 1069–1081
volunteers. Br J Clin Pharmacol 19 : 639–647
Richelson E, Nelson A (1984) Antagonism by antidepressants of
Klamerus KJ, Maloney K, Rudolph RL (1992) Introduction of
neurotransmitter receptors of normal human brain in vitro.
composite parameters to the pharmacokinetics of venlafaxine
and its active metabolites O-desmethyl metabolites. J Clin
Saletu B, Grunberger J, Anderer P, Linzmayer L, Semlitsch HV,
Magni G (1992) Pharmacodynamics of venlafaxine evaluated
Kramer R, Rubicek M, Turner P (1973) The role of norfenfluramine
by EEG brain mapping, psychometry and psychophysiology.
in fenfluramine-induced mydriasis. J Pharm Pharmacol 25 :
Sallee FR, Pollock BG (1990) Clinical pharmacokinetics of
Leung NK-C, Bradshaw CM, Szabadi E (1992) Effect of high ambi-
imipramine and desipramine. Clin Pharmacokinet 18 : 181–184
ent temperature on the kinetics of the pupillary light reflex in
Shur E, Checkley S (1982) Pupil studies in depressed patients : an
healthy volunteers. Br J Clin Pharmacol 33 : 458–460
investigation of the mechanism of action of desipramine. Br J
Loewenfeld IE (1993) The pupil. Wayne State University Press,
Smith SA (1988) Pupillary function in autonomic failure. In :
Millson DS, Haworth SJ, Rushton A, Wilkinson D, Hobson E,
Bannister R (ed) Autonomic failure, 2nd edn. Oxford University
Harry J (1991) The effects of a 5-HT2 receptor antagonist (ICI
169,369) on changes in waking EEG, pupillary responses and
Szabadi E, Bradshaw CM (1986) Antidepressant drugs and the
state of arousal in human volunteers. Br J Clin Pharmacol
autonomic nervous system. In : Deakin JFW (ed) The biology
of depression. Gaskell, London, pp 190–220
Millson DS, Jessup CL, Swaisland A, Haworth S, Rushton A, Harry
Szabadi E, Bradshaw CM (1996) Autonomic pharmacology of α2-
JD (1992) The effects of a selective 5-HT2 receptor antagonist
adrenoceptors. J Psychopharmacol 10 : 6–18
(ICL 170,809) on platelet aggregation and pupillary responses
Szabadi E, Gaszner P, Bradshaw CM (1980) The peripheral anti-
in healthy volunteers. Br J Clin Pharmacol 33 : 281–288
cholinergic activity of tricyclic antidepressants : comparison of
Morley MJ, Bradshaw CM, Szabadi E (1991) Effects of clonidine
amitriptyline in human volunteers. Br J Psychiatry 137 : 433–439
and yohimbine on the pupillary light reflex and carbachol-
Szabadi E, Bradshaw CM, Boston PF, Langley RW (1998) The
evoked sweating in healthy volunteers. Br J Clin Pharmacol
human pharmacology of reboxetine. Hum Psychopharmacol
Mortlock S-A, Langley RW, Bradshaw CM, Szabadi E (1996) Effect
Theofilopoulos N, McDade G, Szabadi E, Bradshaw CM (1995)
of locally applied prazosin on the kinetics of the pupillary light
Effects of reboxetine and desipramine on the kinetics of the
reflex. Br J Clin Pharmacol 42 : 236–238
pupillary light reflex response. Brit J Clin Pharmacol
Muth EA, Haskins JT, Moyer JA (1986) Antidepressant biochem-
ical profile of the novel bicyclic compound Wy-45,030, an ethyl
Wilson WH, Higano H, Papadatos Y, Kelwala S, Ban TA (1983)
cyclohexanol derivative. Biochem Pharmacol 35 : 4493–4497
A double-blind placebo-controlled study to compare the auto-
Patat A, Troy S, Burke J, Trocherie S, Danjou P, Le Coz F, Allain
nomic effects of fluvoxamine with those of amitriptyline
H, Gandon J-M (1998) Absolute bioavailability and electroen-
and doxepine in healthy volunteers. Br J Clin Pharmacol
cephalographic effects of conventional and extended-release for-
mulations of venlafaxine in healthy subjects. J Clin Pharmacol38 : 256–267
Voor in het leger en te paard Als je dacht dat je als ruiter de enige bent die over een paar maanden weer te kampen heeft met aller-hande insecten, die jou en je paard lastigvallen, heb je het mis. Soldaten die uitgezonden worden naar tropische gebieden kampen al jaren met hetzelfde probleem en wel icht met veel ernstiger gevolgen. In samenwerking met het Duitse en Franse lege
 et al. 1986; Richelson 1994). The latter has been
thought to account for venlafaxine’s increased efficacyin severely depressed patients when higher doses are
used (DeMontigny and Preskorn 1995; Preskorn 1995).
et al. 1986; Richelson 1994). The latter has been
thought to account for venlafaxine’s increased efficacyin severely depressed patients when higher doses are
used (DeMontigny and Preskorn 1995; Preskorn 1995).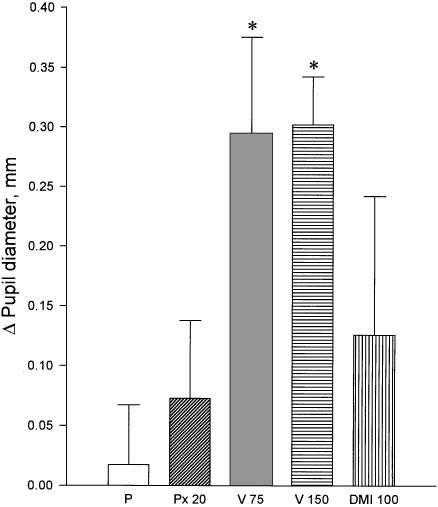 recording of resting pupil diameter and the pupillary light reflex indarkness, in previously dark-adapted eyes. The experimental ses-sion started with three 45-s recordings of resting pupil diameter,the average of which served as the pre-treatment baseline restingpupil diameter. Three hours after ingestion of the first capsule(100 min after ingestion of the second capsule), recordings of rest-ing pupil diameter were repeated and then the pupillary light reflexresponse was studied. The stimuli were six light flashes (green,565 nm peak wavelength) of 200 ms duration, and of incrementalilluminance (measured in the plane of the cornea) : 3.0 × 1093, 8.5 × 1093, 2.5 × 1092, 7.0 × 1092, 0.18, 0.43 mW cm91. The lightflashes were delivered at 25 s intervals, via a light emitting diodepositioned 1 cm from the cornea of the subject’s right eye. Therecordings took place in a dark, sound-attenuated room and thesubjects fixed their gaze on a dim red spot of light positioned approx-imately 2.5 m in front of them. Stimulus presentation was controlledby a microcomputer, and pupillary measures were digitized andstored on a floppy disk for off-line analysis. The parameters stud-ied were : latency (i.e. time elapsing from the onset of the stimulusto the onset of the response, s), amplitude of light reflex response(i.e. the difference between the initial and the minimal diameters ofa pupillary response to a light flash, mm) and 75 % recovery time(i.e. time taken from the peak of the response to obtain 75 % recov-ery, s) (see Fig. 1). Each light reflex response was visually inspected.
recording of resting pupil diameter and the pupillary light reflex indarkness, in previously dark-adapted eyes. The experimental ses-sion started with three 45-s recordings of resting pupil diameter,the average of which served as the pre-treatment baseline restingpupil diameter. Three hours after ingestion of the first capsule(100 min after ingestion of the second capsule), recordings of rest-ing pupil diameter were repeated and then the pupillary light reflexresponse was studied. The stimuli were six light flashes (green,565 nm peak wavelength) of 200 ms duration, and of incrementalilluminance (measured in the plane of the cornea) : 3.0 × 1093, 8.5 × 1093, 2.5 × 1092, 7.0 × 1092, 0.18, 0.43 mW cm91. The lightflashes were delivered at 25 s intervals, via a light emitting diodepositioned 1 cm from the cornea of the subject’s right eye. Therecordings took place in a dark, sound-attenuated room and thesubjects fixed their gaze on a dim red spot of light positioned approx-imately 2.5 m in front of them. Stimulus presentation was controlledby a microcomputer, and pupillary measures were digitized andstored on a floppy disk for off-line analysis. The parameters stud-ied were : latency (i.e. time elapsing from the onset of the stimulusto the onset of the response, s), amplitude of light reflex response(i.e. the difference between the initial and the minimal diameters ofa pupillary response to a light flash, mm) and 75 % recovery time(i.e. time taken from the peak of the response to obtain 75 % recov-ery, s) (see Fig. 1). Each light reflex response was visually inspected.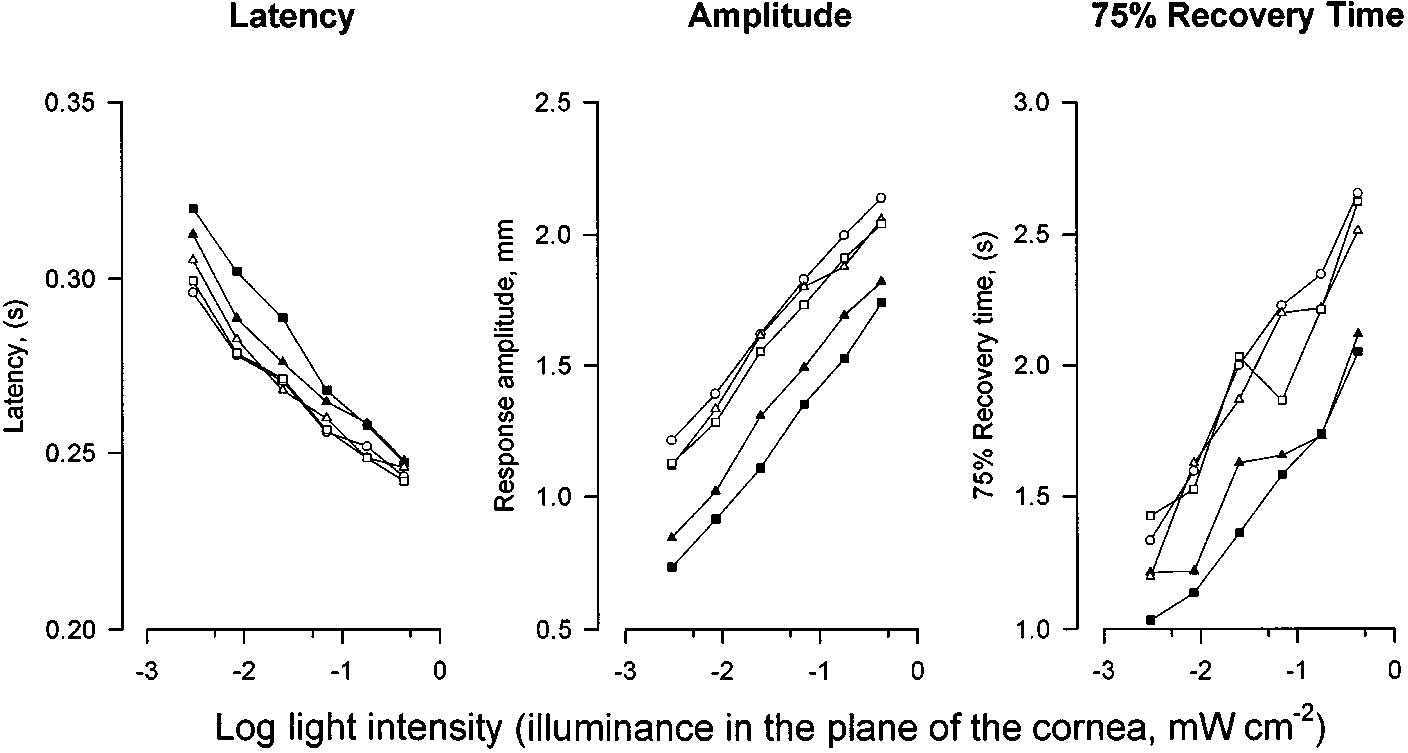
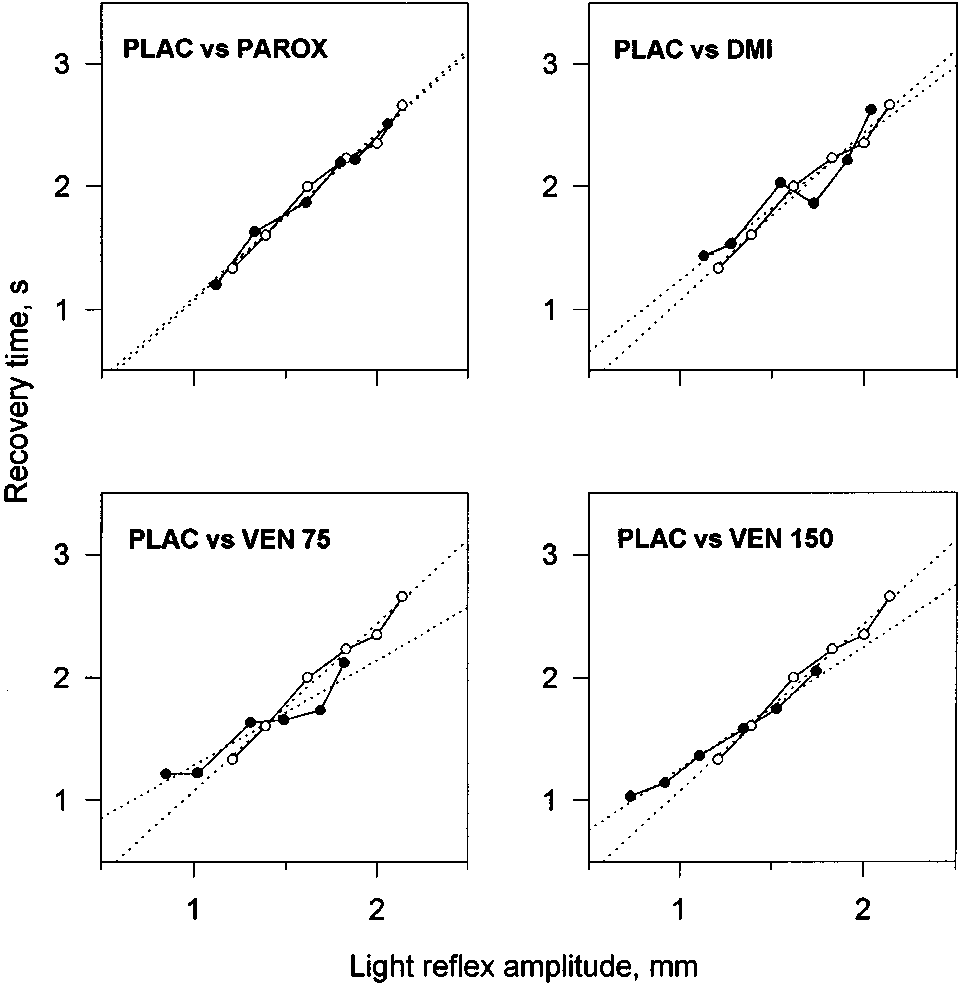 Fig. 3 Parameters of the light
Fig. 3 Parameters of the light