Tadalafil zeigt eine konstante Resorption im Gastrointestinaltrakt, mit maximalen Plasmaspiegeln nach rund zwei Stunden. Der Wirkstoff verteilt sich gut im Gewebe und weist eine hohe Plasmaproteinbindung auf. Seine lange Halbwertszeit erlaubt eine verlängerte Wirkphase. Der Metabolismus erfolgt über das hepatische Enzymsystem CYP3A4, mit der Bildung inaktiver Metaboliten. Exkretion geschieht primär über den Stuhl. Die Häufigkeit von Nebenwirkungen steigt mit der Dosis, wobei vor allem vasodilatatorische Effekte dominieren. Ein gängiger Bezugspunkt in pharmakologischen Analysen ist cialis ohne rezept, das mit dieser Wirkstoffklasse assoziiert ist.
Untitled
Journal of Medical Microbiology (2012), 61, 984–989
Outbreak of pulmonary infection caused byKlebsiella pneumoniae isolates harbouring blaIMP-4and blaDHA-1 in a neonatal intensive care unit inChina
Fangyou Yu,1 Qunhua Ying,2 Chun Chen,3 Tingjian Li,3 Baixing Ding,4Ying Liu,3 Yuanyuan Lu,3 Zhiqiang Qin,5 Chris Parsons,5Cassandra Salgado,5 Di Qu,6 Jingye Pan4 and Liangxing Wang3
1Department of Laboratory Medicine, The First Affiliated Hospital of Wenzhou Medical College,
2Department of Laboratory Medicine, Shaoxing Municipal Women and Children Hospital,
3Department of Respiratory Medicine, The First Affiliated Hospital of Wenzhou Medical College,
4Department of Intensive Care Unit, The First Affiliated Hospital of Wenzhou Medical College,
5Division of Infectious Diseases, Department of Medicine, Medical University of South Carolina,
6Key Laboratory of Medical Molecular Virology of Ministries of Education and Health, Institute of
Medical Microbiology and Institutes of Biomedical Sciences, Shanghai Medical School of FudanUniversity, Shanghai 200032, PR China
Outbreaks caused by Klebsiella pneumoniae producing carbapenemases and other b-lactamases have been reported. Four neonates admitted to a neonatal intensive care unit (NICU)in a Chinese hospital developed respiratory infection while receiving intensive care. In all fourcases, multidrug-resistant K. pneumoniae was isolated from multiple respiratory specimens,leading to additional characterization of these organisms and investigation of the localenvironment in the NICU. Multiple b-lactamase genes, including blaTEM-1, blaIMP-4, blaDHA-1 andblaCTX-M-14, as well as the quinolone resistance gene qnrB4, were harboured by transferableplasmids from all four clinical isolates. Furthermore, PFGE confirmed that three of the four clinicalisolates from the patients and three K. pneumoniae isolates collected from the hands of health-care workers and an incubator in the NICU belonged to the same PFGE cluster, indicating that anoutbreak due to multidrug-resistant K. pneumoniae carrying blaIMP-4 and blaDHA-1 occurred in thisNICU. As far as is known, this is the first report of the co-existence of blaIMP-4 and blaDHA-1 in thesame K. pneumoniae isolate. These data suggest that additional precautions are needed to
prevent outbreaks of infection caused by multidrug-resistant K. pneumoniae resulting from
). Carbapenems or fluoroquino-lones are often used for the treatment of clinical infections
Klebsiella pneumoniae frequently exhibits resistance to
caused by this organism. However, resistance of K. pneumo-
extended-spectrum cephalosporins due to the production
of extended-spectrum b-lactamases (ESBLs)
), and this is often due to theproduction of carbapenemases, particularly K. pneumoniae
Abbreviations: CLSI, Clinical and Laboratory Standards Institute; ESBL,
carbapenemases (KPCs) and class B metallo-b-lactamases
carbapenemase; MBL, class B metallo-b-lactamase; NICU, neonatal
NICU outbreak of carbapenemase-producing K. pneumoniae
been found in members of the Enterobacteriaceae worldwide
Antimicrobial susceptibility testing. Antimicrobial susceptibilities
were determined initially using GNS cards of the Vitek system
to the family Enterobacteriaceae, KPCs have emerged in non-
(bioMe´rieux). Multidrug resistance profiles were then furtherevaluated by a disc diffusion test using commercial discs containing
cefazolin (30 mg), cefotaxime (30 mg), ceftazidime (30 mg), cefepime
(30 mg), aztreonam (30 mg), cefoxitin (30 mg), imipenem (10 mg),
dominant carbapenemase and has been recognized in many
meropenem (10 mg), chloramphenicol (30 mg), tetracycline (30 mg),
members of the Enterobacteriaceae, such as K. pneumoniae,
trimethoprim/sulfamethoxazole (1.25/23.75 mg), amikacin (30 mg),
Serratia marcescens, Escherichia coli and Enterobacter cloacae
gentamicin (10 mg), ciprofloxacin (5 mg) and levofloxacin (5 mg).
An agar dilution method was used to determine MIC values
including IMP and VIM, are commonly harboured by
according to the criteria recommended by the Clinical and
non-fermentative bacteria and have recently been iden-
Laboratory Standards Institute E. coli ATCC 25922was used as a quality control strain for antimicrobial susceptibility
tified in members of the Enterobacteriaceae worldwide
(; ). MBLs often confer high-level resistance to all b-
Detection of b-lactamases. A modified Hodge test was performed
lactams except aztreonam and are not inhibited by
to detect carbapenemases, as described previously A
clavulanic acid, tazobactam or sulbactam. Although
double-disc synergy test was designed to detect MBLs, as described by
several IMP- and VIM-type MBLs have been described
All the isolates studied were tested for ESBL
in China, most were found in non-fermentative Gram-
production by the CLSI-recommended confirmatory double-disccombination test
negative bacilli (. Recent data indicatethat IMP-4 confers reduced susceptibility to carbapenems
Detection of antimicrobial resistance determinants. Total DNA
for K. pneumoniae isolated from patients in China (
was extracted by boiling. Potential antimicrobial resistance determi-
nants, which included carbapenemase genes, ESBL genes, plasmid-
clinical strains of K. pneumoniae carrying plasmid-borne
borne ampC genes and plasmid-borne quinolone resistance determi-
nants, were investigated by PCR and nucleotide sequencing, using
IMP-4, blaSHV-12 and armA were found at a paediatric
gene was also found to co-exist with blaKPC-2 in K.
ompK36 genes were determined by PCR and DNA sequencing with
primers ompK35-F (59-ATGATGAAGCGCAATATTCTGGCAGTGG-39),
ompK35-R (59-TCGGCTTTGTCGCCATTGCCGTCA-39), ompK36-F
producing IMP-4 found in China were clonally unrelated
(59-ATGAAAGTTAAAGTACTGTCCCTC-39) and ompK36-R (59-
and occurred sporadically. An outbreak caused by multi-
GTCGTCGGTAGAGATACCGGC-39). All amplicon sequences were
drug-resistant K. pneumoniae harbouring bla
compared with the sequences available in GenBank (http://www.
been found previously in China. In this report, we
describe an outbreak of multidrug-resistant K. pneumo-
Transfer of carbapenem resistance determinants. In order to
niae infection in a neonatal intensive care unit (NICU) in
determine whether carbapenem resistance was transferable in K.
China, as well as isolation of related organisms from
pneumoniae isolates, a conjugation experiment was carried out in
Luria–Bertani broth with E. coli J53 as the recipient, as describedpreviously Transconjugants were selected ontryptic soy agar plates containing sodium azide (100 mg ml21) for
counterselection and imipenem (0.5 mg ml21) for plasmid-mediatedcarbapenem resistance selection.
Isolation and identification of bacterial strains. From October toDecember 2010, four neonates with asphyxia were admitted to the
Determination of the flanking regions of the blaIMP-4 gene.
NICU of the 400-bed Shaoxing Municipal Women and Children
Plasmid DNA of the transconjugants was extracted using a Plasmid
Hospital in Shaoxing, eastern China. Of note, hospital admission for
Midi kit (Qiagen) according to the manufacturer’s instructions.
all four patients (designated patients 1–4) overlapped. Before
Purified blaIMP-bearing conjugative plasmids extracted from the
admission to the NICU, pulmonary infections diagnosed by physical
transconjugants were sequenced directly using a series of outward-
examination and new findings consistent with pneumonia on chest
directed primers specific for the locations next to the blaIMP-4
radiography were not found among the four patients. Bacterial
isolates from sputum specimens growing over more than three-quarters of the plate by quantitative culture were considered to be
PFGE. Genomic DNA was prepared from all tested K. pneumoniae
responsible for the pulmonary infection. Bacterial isolates were
isolates and cleaved with 40 U XbaI. Electrophoresis was performed
identified by a Vitek-32 microbiology analyser (bioMe´rieux) accord-
on 1 % agarose gels in 0.5 M Tris/borate/EDTA buffer on a CHEF-
ing to the manufacturer’s instructions and additional biochemical
Mapper XA PFGE system (Bio-Rad) for 24 h at 14 uC, with run
tests. The initial K. pneumoniae isolates were screened for further
conditions of 6 V cm21, a pulse angle of 120u and pulse times of
investigation. After K. pneumoniae was isolated from patient 4, an
5–20 s. A l DNA ladder (Amersham Biosciences) was used as a
outbreak control team was organized and infection control measures
molecular mass marker and DNA bands were stained with
were implemented. Environmental samples were obtained for culture
ethidium bromide (0.5 mg ml21) prior to identification by
by rubbing sterile polyester-fibre-tipped swabs moistened with sterile
photography under UV light. Band profiles were interpreted by
saline repeatedly over designated sites in the immediate vicinity of the
the criteria of Patterns with a difference of no
patients, including equipment used for their care and the fingers of
more than three DNA bands were considered to belong to the same
medical staff caring for the patients.
hospital on day 46. Although the isolates KpSX2, KpSX3and KpSX4 exhibited low-level resistance to imipenem,
A suspected lung infection was diagnosed in patient 1 (aged
patients 2, 3 and 4 were treated with intravenous imipenem
16 days), patient 2 (aged 17 days), patient 3 (aged 22 days)
(20 mg kg21 every 12 h) for 10–14 days and left the
and patient 4 (aged 14 days). K. pneumoniae isolates
hospital on days 44, 47 and 40, respectively, after multi-
designated KpSX1– KpSX4 were first recovered from
drug-resistant K. pneumoniae was no longer isolated and
sputum specimens of patients 1–4 following hospitalization
the symptoms of lung infection had disappeared.
for 22, 22, 32 and 16 days, respectively. Subsequently, K. pneumoniae isolates with identical antimicrobial resistance
All tested isolates harboured int1, blaSHV, blaTEM, blaIMP,
patterns were isolated from the sputum of each patient more
blaDHA, blaCTX-M and qnrB4 genes detected by PCR. Addi-
than three times. The gestational ages of the four patients
tional sequencing of the amplified PCR products revealed
ranged from 26 to 29 weeks and their weights were only
the presence of blaSHV-11, blaTEM-1, blaIMP-4, blaDHA-1,
1050–1370 g both of these are risk factors for the
blaCTX-M-14 and qnrB4 among these isolates. Therefore, co-
acquisition of hospital-associated infections. Three K.
existence of multiple b-lactamase genes within each
pneumoniae isolates designated KpE1, KpE2 and KpE3 were
individual isolate could explain the resistance of these
recovered from environmental samples, comprising two
isolates to all b-lactams tested. To the best of our
from the fingers of two different nurses and one from an
knowledge, this is the first report of the co-existence of
blaIMP-4 and blaDHA-1 in the same K. pneumoniae isolate.
Apart from multidrug-resistant K. pneumoniae, other
Detection of multiple b-lactamases produced by members of
multidrug-resistant pathogens, such as meticillin-resistant
the Enterobacteriaceae in the clinical laboratory is challeng-
Staphylococcus aureus, ESBL-producing Enterobacteriaceae,
ing. The lack of ESBLs in the present study could be
vancomycin-resistant enterococci and multidrug-resistant
attributable to the masking effect of co-production of ESBLs,
Acinetobacter baumannii, were not isolated from the
AmpCs and carbapenemases. For example, co-production of
clinical specimens including stools of the four investigated
KPCs and MBLs masked the results of EDTA- or boronic
patients. Each of the four clinical isolates and the three
environmental isolates was susceptible to amikacin but
carbapenemase-producing members of the Enterobacteria-
resistant to cefazolin, ceftazidime, cefotaxime, cefepime,
ceae also exhibit low-level resistance or even susceptibility to
aztreonam, cefoxitin, gentamicin, tetracycline, chlor-
amphenicol and trimethoprim/sulfamethoxazole
decreased susceptibility of our isolates to ciprofloxacin could
as determined by a disc diffusion test according to the
be explained by the existence of qnrB4.
criteria of the Apart from KpSX1, whichexhibited no zones of inhibition, all tested isolates
b-Lactam resistance could be transferred by conjugation
exhibited similar zones of inhibition and MIC values for
from all K. pneumoniae isolates to their recipients. All trans-
IMP and MEM (According to the interpretive
conjugants harboured int1, blaTEM-1, blaIMP-4, blaDHA-1,
standards for IMP and MEM for Enterobacteriaceae
blaCTX-M-14 and qnrB4 but not blaSHV-11. The E. coli
transconjugants also exhibited relatively low MICs for IMP
resistant to IMP and MEM. A modified Hodge test was
and MEM that were insufficient to explain the carbapenem
positive for all tested isolates, indicating that these isolates
resistance exhibited by the parental isolates. Therefore, we
produced carbapenemases. However, all tested isolates
sought to identify additional mechanisms for carbepenem
were negative for MBLs determined by a double-disc
synergy test and negative for ESBLs determined by the
IMP-4 MBL production combined with loss of outer-
CLSI-recommended double-disc test ). Prior to
membrane proteins confers high-level resistance to carba-
the recovery of multidrug-resistant K. pneumoniae isolates,
all four patients were treated with intravenous mezlocillin
we sought to identify resistance determinants within the
(75 mg kg21 every 12 h) plus cefmetazole (50 mg kg21
ompK35 and ompK36 genes for our K. pneumoniae isolates.
every 12 h) for preventing infections, and patient 1 was
The nucleotide sequences of the ompK35 genes of all seven
treated additionally with intravenous panipenem (20 mg
isolates were identical to that of carbapenem-susceptible K.
kg21 every 12 h) after the suspected lung infection was
pneumoniae ATCC 13883. A CAT mutation was observed
found. Treatment with intravenous cephalosporins or car-
at nt 160 in the ompK36 gene for isolate KpSX1, resulting
bepenems may facilitate increased colonization by resistant
in initiation of a stop codon at position 54 (CAGATAG)
K. pneumoniae, which can subsequently cause infection.
for this strain. An early termination of translation caused
After multidrug-resistant K. pneumoniae isolates were
by the CAT mutation at nt 160 in the ompK36 gene might
identified, patient 1 was treated with intravenous amikacin
lead to the loss of OmpK36. These data indicated that high-
(7.5 mg kg21 every 24 h) and levofloxacin (10 mg kg21
level resistance of KpSX1 to IMP and MEM may be due to
every 24 h) for 10 days according to the results of
the combination of IMP-4 and deficiency of the porin.
antimicrobial susceptibility testing. Thereafter, multidrug-resistant K. pneumoniae was not isolated and the symptoms
We found that blaIMP-4 was located within a class I inte-
of lung infection disappeared in patient 1, who left the
gron whose order was int1-blaIMP-4-orfII-orfIII-qacED1-sul1.
Table 1. Phenotypic and genotypic characteristics of the K. pneumoniae clinical and environmental isolates
DGA, Gestational age of patient. dATM, Aztreonam; C, chloramphenicol; CAZ, ceftazidime; CEC, cefaclor; CTX, cefotaxime; CZ, cefazolin; FEP, cefepime; FOX, cefoxitin; GEN, gentamicin; IMP, imipenem; MEM, meropenem;SXT, trimethoprim/sulfamethoxazole; TE, tetracycline. §+, Positive. ||AMC, Amoxicillin plus clavulanic acid; AMK, amikacin; CMZ, cefmetazole; LEV, levofloxacin; MEZ, mezlocillin; PAP, panipenem.
Bradford, P. A., Bratu, S., Urban, C., Visalli, M., Mariano, N.,
Landman, D., Rahal, J. J., Brooks, S., Cebular, S. & Quale, J.
(2004). Emergence of carbapenem-resistant Klebsiella species posses-
sing the class A carbapenem-hydrolyzing KPC-2 and inhibitor-
resistant TEM-30 b-lactamases in New York City. Clin Infect Dis 39,
Cai, J. C., Zhou, H. W., Zhang, R. & Chen, G.-X. (2008). Emergence ofSerratia marcescens, Klebsiella pneumoniae, and Escherichia coli isolates
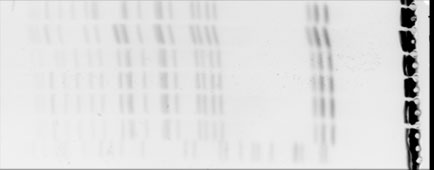
Fig. 1. PFGE patterns for the K. pneumoniae strains. The
possessing the plasmid-mediated carbapenem-hydrolyzing b-lacta-
restriction enzyme XbaI was used for genomic DNA digestion.
mase KPC-2 in intensive care units of a Chinese hospital. AntimicrobAgents Chemother 52, 2014–2018.
Chen, L.-R., Zhou, H.-W., Cai, J.-C., Zhang, R. & Chen, G.-X. (2009).
The flanking structure of blaIMP-4 was therefore identical to
Combination of IMP-4 metallo-b-lactamase production and porin
the nucleotide sequence of a class I integron harbouring
deficiency causes carbapenem resistance in a Klebsiella oxytoca clinical
isolate. Diagn Microbiol Infect Dis 65, 163–167.
(GenBank accession no. FJ384365) described
previously in Shanghai near to Shaoxing, China
CLSI (2011). Performance Standards for Antimicrobial Susceptibility
The genetic relatedness of all K. pneumoniae isolates
Testing; 21st Informational Supplement. M100-S21. Wayne, PA:
was also evaluated using PFGE. These results showed that
Clinical and Laboratory Standards Institute.
two different band patterns, designated types A and B, were
Cuzon, G., Naas, T., Villegas, M. V., Correa, A., Quinn, J. P. &
identified for these isolates. PFGE type A accounted for three
Nordmann, P. (2011). Wide dissemination of Pseudomonas aeruginosaproducing b-lactamase bla
clinical isolates (KpSX1, KpSX2 and KpSX3) and all three
KPC-2 gene in Colombia. Antimicrob Agents
environmental isolates, whilst KpSX4 exhibited PFGE type B
Espedido, B., Iredell, J., Thomas, L. & Zelynski, A. (2005). Wide
These data indicated that, with the exception of
dissemination of a carbapenemase plasmid among Gram-negative
KpSX4, all of the isolates recovered in this study were closely
bacteria: implications of the variable phenotype. J Clin Microbiol 43,
Our data complement those reported in recent outbreaks
Falagas, M. E. & Karageorgopoulos, D. E. (2009). Extended-
caused by K. pneumoniae producing carbapenemases and
spectrum b-lactamase-producing organisms. J Hosp Infect 73, 345–354.
other b-lactamases as described elsewhere ;
Gupta, N., Limbago, B. M., Patel, J. B. & Kallen, A. J. (2011). Carbapenem-resistant Enterobacteriaceae: epidemiology and preven-
Ultimately, all four patients were isolated in single-bed
rooms, where strict contact precautions were implemented.
Kassis-Chikhani, N., Decre´, D., Ichai, P., Sengelin, C., Geneste, D.,
All NICU personnel were provided with additional training
Mihaila, L., Dussaix, E. & Arlet, G. (2010). Outbreak of Klebsiella
regarding standard precautions for prevention of infections
pneumoniae producing KPC-2 and SHV-12 in a French hospital.
in this setting, including appropriate hand hygiene and
J Antimicrob Chemother 65, 1539–1540.
meticulous environmental cleaning. In addition, incuba-
Liu, Y., Zhang, B., Cao, Q., Huang, W., Shen, L. & Qin, X. (2009). Two
tors, telephones, personal computers and door handles
clinical strains of Klebsiella pneumoniae carrying plasmid-borne
were cleaned with approved environmental disinfectants.
blaIMP-4, blaSHV-12, and armA isolated at a pediatric center in
Since the implementation of these procedures, multidrug-
Shanghai, China. Antimicrob Agents Chemother 53, 1642–1644.
resistant K. pneumoniae isolates have not been isolated
Maltezou, H. C. (2009). Metallo-b-lactamases in Gram-negative
from patients or environmental sources in this NICU. We
bacteria: introducing the era of pan-resistance? Int J Antimicrob
recommend early implementation of outbreak investi-
gations with identification of two or more clinical cases of
Mendes, R. E., Bell, J. M., Turnidge, J. D., Yang, Q., Yu, Y., Sun, Z. &
multidrug-resistant K. pneumoniae in the NICU setting in
Jones, R. N. (2008). Carbapenem-resistant isolates of Klebsiella
order to prevent additional cases and morbidity associated
pneumoniae in China and detection of a conjugative plasmid (blaKPC-2
with these clinically challenging infections.
plus qnrB4) and a blaIMP-4 gene. Antimicrob Agents Chemother 52,798–799.
In conclusion, our data suggest that an outbreak due to
Nordmann, P., Cuzon, G. & Naas, T. (2009). The real threat of
multidrug-resistant K. pneumoniae occurred in this NICU.
Klebsiella pneumoniae carbapenemase-producing bacteria. LancetInfect Dis 9, 228–236.
Peleg, A. Y., Franklin, C., Bell, J. M. & Spelman, D. W. (2005).
Dissemination of the metallo-b-lactamase gene blaIMP-4 amongGram-negative pathogens in a clinical setting in Australia. Clin
We are grateful to Dr Rong Zhang from the second affiliated hospital
of Zhejiang University for PFGE technical assistance. This work wassupported by the 11th Five-Year Plan of the Ministry of Sciences and
Queenan, A. M. & Bush, K. (2007). Carbapenemases: the versatile
Technology (2010DFA32100, 2009ZX09303-005 and 2008ZX10003-
b-lactamases. Clin Microbiol Rev 20, 440–458.
016) and the Scientific Technology Development Foundation of
Robicsek, A., Strahilevitz, J., Sahm, D. F., Jacoby, G. A. & Hooper,
Shanghai (08JC1401600, 10410700600).
D. C. (2006). qnr prevalence in ceftazidime-resistant Enterobacteriaceae
NICU outbreak of carbapenemase-producing K. pneumoniae
isolates from the United States. Antimicrob Agents Chemother 50, 2872–
Walsh, T. R., Toleman, M. A., Poirel, L. & Nordmann, P. (2005).
Metallo-b-lactamases: the quiet before the storm? Clin Microbiol Rev
Robledo, I. E., Aquino, E. E. & Va´zquez, G. J. (2011). Detection of the
KPC gene in Escherichia coli, Klebsiella pneumoniae, Pseudomonas
Wang, M., Tran, J. H., Jacoby, G. A., Zhang, Y., Wang, F. & Hooper,
aeruginosa, and Acinetobacter baumannii during a PCR-based
D. C. (2003). Plasmid-mediated quinolone resistance in clinical
nosocomial surveillance study in Puerto Rico. Antimicrob Agents
isolates of Escherichia coli from Shanghai, China. Antimicrob Agents
Wei, Z.-Q., Du, X.-X., Yu, Y.-S., Shen, P., Chen, Y.-G. & Li, L.-J. (2007).
Poulakou, G., Panagea, T., Vourli, S., Zerva, L., Armaganidis, A. &
Plasmid-mediated KPC-2 in a Klebsiella pneumoniae isolate from
other authors (2010). An outbreak of infection due to b-lactamase
China. Antimicrob Agents Chemother 51, 763–765.
Klebsiella pneumoniae carbapenemase 2-producing K. pneumoniae in
Wei, Z., Yu, T., Qi, Y., Ji, S., Shen, P., Yu, Y. & Chen, Y. (2011).
a Greek university hospital: molecular characterization, epidemiology,and outcomes. Clin Infect Dis 50, 364–373.
Coexistence of plasmid-mediated KPC-2 and IMP-4 carbapenemasesin isolates of Klebsiella pneumoniae from China. J Antimicrob
Steinmann, J., Kaase, M., Gatermann, S., Popp, W., Steinmann, E.,
Damman, M., Paul, A., Saner, F., Buer, J. & Rath, P. (2011). Outbreakdue to a Klebsiella pneumoniae strain harbouring KPC-2 and VIM-1
Wu, Q., Liu, Q., Han, L., Sun, J. & Ni, Y. (2010). Plasmid-mediated
in a German university hospital, July 2010 to January 2011. Euro
carbapenem-hydrolyzing enzyme KPC-2 and ArmA 16S rRNA
methylase conferring high-level aminoglycoside resistance in carba-penem-resistant Enterobacter cloacae in China. Diagn Microbiol Infect
Tenover, F. C., Arbeit, R. D., Goering, R. V., Mickelsen, P. A., Murray,
B. E., Persing, D. H. & Swaminathan, B. (1995). Interpretingchromosomal DNA restriction patterns produced by pulsed-field
Yu, Y., Ji, S., Chen, Y., Zhou, W., Wei, Z., Li, L. & Ma, Y. (2007).
gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol
Resistance of strains producing extended-spectrum b-lactamases and
genotype distribution in China. J Infect 54, 53–57.
Villegas, M. V., Lolans, K., Correa, A., Kattan, J. N., Lopez, J. A., Quinn,
Zioga, A., Miriagou, V., Tzelepi, E., Douzinas, E., Tsakiri, M., Legakis,
J. P. & Colombian Nosocomial Resistance Study Group (2007).
N. J., Daikos, G. L. & Tzouvelekis, L. S. (2010). The ongoing challenge
First identification of Pseudomonas aeruginosa isolates producing a
of acquired carbapenemases: a hospital outbreak of Klebsiella
KPC-type carbapenem-hydrolyzing b-lactamase. Antimicrob Agents
pneumoniae simultaneously producing VIM-1 and KPC-2. Int J
2013 Preventive Drug List For High-Deductible Health Plans Only effective 1/1/13 If your High-Deductible Health Plan includes the Preventive Drug List option, you just pay a copay for preventive care medications instead of having to meet your plan’s deductible for certain prescription drugs. Prescription drugs on the Preventive Drug List will be covered as if you already met your dedu
THIS WON’T HURT A BIT: Why the vaccine crisis shows we shouldn’t believe what health “planners” tell us about how to reform drug policy JULIA WITT BRIAN FERGUSON AIMS COMMENTARY Atlantic Institute for Market Studies The Atlantic Institute for Market Studies (AIMS) is an independent, non-partisan, social and economic policythink tank based in Halifax. The Institute was
 Bradford, P. A., Bratu, S., Urban, C., Visalli, M., Mariano, N.,
Landman, D., Rahal, J. J., Brooks, S., Cebular, S. & Quale, J.
Bradford, P. A., Bratu, S., Urban, C., Visalli, M., Mariano, N.,
Landman, D., Rahal, J. J., Brooks, S., Cebular, S. & Quale, J.