Tadalafil zeigt eine konstante Resorption im Gastrointestinaltrakt, mit maximalen Plasmaspiegeln nach rund zwei Stunden. Der Wirkstoff verteilt sich gut im Gewebe und weist eine hohe Plasmaproteinbindung auf. Seine lange Halbwertszeit erlaubt eine verlängerte Wirkphase. Der Metabolismus erfolgt über das hepatische Enzymsystem CYP3A4, mit der Bildung inaktiver Metaboliten. Exkretion geschieht primär über den Stuhl. Die Häufigkeit von Nebenwirkungen steigt mit der Dosis, wobei vor allem vasodilatatorische Effekte dominieren. Ein gängiger Bezugspunkt in pharmakologischen Analysen ist cialis ohne rezept, das mit dieser Wirkstoffklasse assoziiert ist.
Porodnice.cz
Journal of Obstetrics and Gynaecology (September 2003) Vol. 23, No. 5, 469–478
Evidence-based labour ward guidelines for thediagnosis, management and treatment ofspontaneous preterm labour
R. F. LAMONT1 and the INTERNATIONAL PRETERM LABOUR COUNCIL2
1Department of Obstetrics and Gynaecology, Northwick Park Hospital, Harrow, UK
and Tressler, 2001). Delaying delivery may reduce the rate
Currently, there is considerable variation in the way spontaneous
of long-term morbidity by facilitating the growth and
preterm labour is diagnosed and managed internationally. As a
maturation of developing organs and system. The benefits
result, 12 international leading experts from 10 countries met to
of administration of antepartum glucocorticoids (Crowley
establish consensus on clinical recommendations and guidelines
et al., 1990) to reduce the incidence and severity of
regarding the diagnosis, management and treatment of spontaneouspreterm labour. The consensus was supported by evidence from
respiratory distress syndrome may be exploited by delay.
quality literature published during the last 15 years and graded
Delay may also permit transfer of the fetus in utero to a
using the National Health Service Executive classification system
centre with neonatal intensive care unit facilities (Lamont et
(Grades A – C), endorsed by the Royal College of Obstetricians and
Gynaecologists. The Council found enough evidence of a lack of a
The economic burden of preterm birth includes the
consensus across nations to recommend guidelines. It is hoped that
immediate neonatal intensive care unit costs together with
these international guidelines, while not meant to be prescriptive,
the longer-term costs for residential care or support of
will initiate discussion and correspondence for a basis for
infants born preterm with residual disabilities. In the United
implementation on a national level and be adapted for local clinical
States, the weekly cost of caring for a baby in the neonatal
practice, leading to further meetings around the world, to discuss
intensive care unit is estimated to be approximately
other areas including infection, mode of delivery and in-uterotransfer.
US$10 000 per baby (Keirse, 1995). Annually this amountsto approximately US$5 000 000 000. If, as a result of
disability, an infant needs long-term residential care, thelifelong cost may be as high as US$450 000 each.
Preterm birth, defined as delivery 5 37 completed weeks of
pregnancy (World Health Organisation, 1993) has a world-
spontaneous preterm labour is diagnosed, managed and
wide incidence estimated to be 13 million, occurring in 5 –
treated internationally and this variation is outlined in
10% of all pregnancies (Hall et al., 1997). Preterm birth is
Table I. The existence of national guidelines varies from
not only one of the more common obstetric complications,
country to country with little or no agreement on the use of
but also one of the most serious causes of perinatal
mortality and morbidity. Early preterm birth ( 5 32 weeks’
In this review, the guidelines for diagnosis concentrated
gestation) is associated with a high perinatal mortality rate
on whether the woman was in true labour and whether it
was at a gestational age that required intervention. The
The second and third trimesters of pregnancy are vital for
diagnostic criteria were based on contractions, cervical
maturation of the fetal lungs and other organs in
dilatation and cervical effacement, and consideration was
preparation for extrauterine life. If this is interrupted by
given to the role of oncofetal fibronectin and vaginal
very early delivery, the chances of survival of the newborn
ultrasound measurements of cervical length. The issues
are markedly diminished. Preterm birth is also the leading
surrounding the choice of tocolytic focused on licensed
cause of long-term morbidity, including neurodevelopmen-
drugs including the oxytocin antagonist, atosiban, and b-
tal handicap, cerebral palsy, seizure disorders, blindness,
agonists, as well as unlicensed drugs. The relative efficacy
deafness and non-neurological disorders, such as broncho-
and safety of each class were compared, contrasted and
pulmonary dysplasia and retinopathy of prematurity (Hole
graded with respect to quality of evidence, according to
2International Preterm Labour Council: Dr Anders Atke; Holbæk Sygehus, Denmark; Dr Jim van Eyck; Isala, Klinieken Locatie, Sophia, the
Netherlands; Dr Hanns Helmer; University of Vienna, Austria; Professor Ingemar Ingemarsson; Lund University Hospital, Sweden; Dr RonnieLamont (Chair); Northwick Park Hospital, United Kingdom; Dr Line Leduc; University of Montreal, Canada; Professor Jean-Marie Moutquin;University of Montreal, Canada; Professor Nicola Rizzo; University of Bologna, Italy; Dr Jens Svare; University of Copenhagen, Denmark;
Professor Arthur Wischnik; Augsburg Central Clinic, Germany. Additional contributions: Professor Cabero Roura; Hospital Materno-InfantilValle Hebro´n Barcelona, Spain; Professor Dominique Cabrol; Groupe Hospitalier Cochin, France. Correspondence to: Dr Ronnie Lamont, Department of Obstetrics and Gynaecology, Northwick Park Hospital, Watford Road, Harrow,Middlesex HA1 3UJ, UK. Tel: 0044 20 8869 2862Fax: 0044 20 8869 2864.
ISSN 0144-3615 print/ISSN 1364-6893 online/03/050469-10 ª Taylor & Francis Limited, 2003DOI: 10.1080/0144361031000153666
Table I. Current clinical practice for the prevention of preterm labour in Europe and Canada
Gynaecology, since 1997,due to be revised
*Societa` Italiana di Ginecologia e Ostetricia (SIGO); {Oesterreichische Gesellschaft fuer Gynaekologie und Geburtshilfe (OeGGG);{Sociedad Espan˜ola de Ginecologı´a y Obstetricia (SEGO); §Royal College of Obstetricians and Gynaecologists (RCOG); **CollegeNational des Gynecologues et Obstetriciens Francais (CNGOF).
recognised definitions. The absolute and relative contra-
the literature that supplied evidence of an appropriate
indications for prolongation of pregnancy were also
quality published during the last 15 years.
To ensure that the evidence used to support the
The development of clinical guidelines requires an
statements was based on current research, the evidence for
evidence-based approach to improve patient outcome and
diagnosis and treatment of spontaneous preterm labour was
allow more efficient use of resources (Woolf et al., 1999).
graded following the United Kingdom National Health
With recent advances in our understanding of the aetiology
System Executive classification system (which is endorsed
and mechanisms of spontaneous preterm labour and the
by the Royal College of Obstetricians and Gynaecologists.
availability of safer, more specific tocolytics, it was felt that
guidelines should be developed to achieve, if possible, an
Grade A evidence is derived from randomised controlled
international consensus in patient diagnosis, management
trials or systematic reviews of randomised trials. Meta-
and treatment. The aim of this report is to provide evidence-
analyses/systematic reviews had to include 50% or more
based practical guidelines for the diagnosis, management
and treatment of spontaneous preterm labour within a
Grade B evidence is from non-randomised controlled
labour ward environment. It is hoped that these guidelines
trials, other robust experimental or good observational
will stimulate thought and debate internationally with
respect to the management of spontaneous preterm labour
4 50% randomised controlled studies.
and be used as a basis for the development of national and
Grade C evidence is more limited and refers to
observational studies with poorer methodology or casereports or the advice relies on consensus amongprofessional groups.
MethodsIn June 2001, a group of 10 obstetricians with a special
Within each literature search only certain papers were
interest in the management of preterm labour convened
selected for grading. Evidence for oncofetal fibronectin and
under the auspices of the ‘International Preterm Labour
transvaginal ultrasound scanning concentrated on papers
Council’ to discuss clinical guidelines for the diagnosis,
that investigated these markers for the prediction of preterm
birth rather than predicting infection. Evidence for
corticosteroid recommendations concentrated on papers
Their objective was: ‘to reduce the fetomaternal mortality
that examined single and/or repeated doses of therapy and
and morbidity associated with spontaneous preterm labour
those papers whose outcome measures concentrated on the
and preterm birth’. Their discussions focused on the
evidence for decreasing fetal mortality and respiratory
diagnosis and management of spontaneous preterm labour
distress syndrome. Evidence for the benefits of tocolytic
within the labour ward. The recommendations were
therapy came from those papers that looked at placebo-
supported by data collected from a systematic review of
controlled trials or comparisons between tocolytics.
International preterm labour council guidelines
fibronectin has a high negative predictive value of 86.6%
The following databases were used to ensure that the
for preterm delivery before 37 weeks’ gestation so may
prevent unnecessary intervention but has a low positive
MEDLINE (1986 – present), EMBASE (1986 – present),
predictive value of 45.2% for delivery (Grade A) (Rozen-
BIOSIS (1986 – present), Current Contents (1995 – present),
Derwent Drugfile (1986 – present), Reactions Database
When compared with digital examination and transab-
(1986 – present). The search terms were: ‘steroid’/‘cortico-
dominal scanning, transvaginal ultrasound has a high
steroid’, ‘preterm labour’/‘labour premature’, ‘randomised’,
sensitivity for the detection of cervical shortening and the
‘meta-analysis’, ‘controlled trial’, ‘utero AND transfer
risk of preterm birth (Vause and Johnston, 2000). Grade A
AND guideline’, ‘fetal fibronectin AND ultrasound’,
evidence indicates that ultrasound measurement of cervical
‘tocolysis’/‘tocolytic AND efficacy’, ‘safety AND mater-
length is more valuable than the Bishop score for predicting
the onset of spontaneous labour within 7 days, whenmeasured close to term (Rozenberg et al., 1999). There isstill debate with respect to the length of the cervix below
which the risk of preterm birth is increased and by how
The discussion and data from the systematic literature
much this risk is increased, if at all, with shorter cervical
review are presented in the form of the following
subheadings: the diagnosis of spontaneous preterm labour,
It was concluded that fetal fibronectin and transvaginal
the management and treatment of spontaneous preterm
ultrasound used for the diagnosis of spontaneous preterm
labour (tocolytic therapy, the administration of antepartum
labour as an adjuvant to clinical parameters but without
glucocorticoids, the role of infection and preterm labour
further research should not be recommended for routine
and other measures) and finally the contraindications for
use. It was resolved to consider the use of fetal fibronectin
the intervention of spontaneous preterm labour.
and transvaginal ultrasound in the diagnosis of spontaneouspreterm labour and their place in the prediction andprevention of preterm birth, as part of future guidelines.
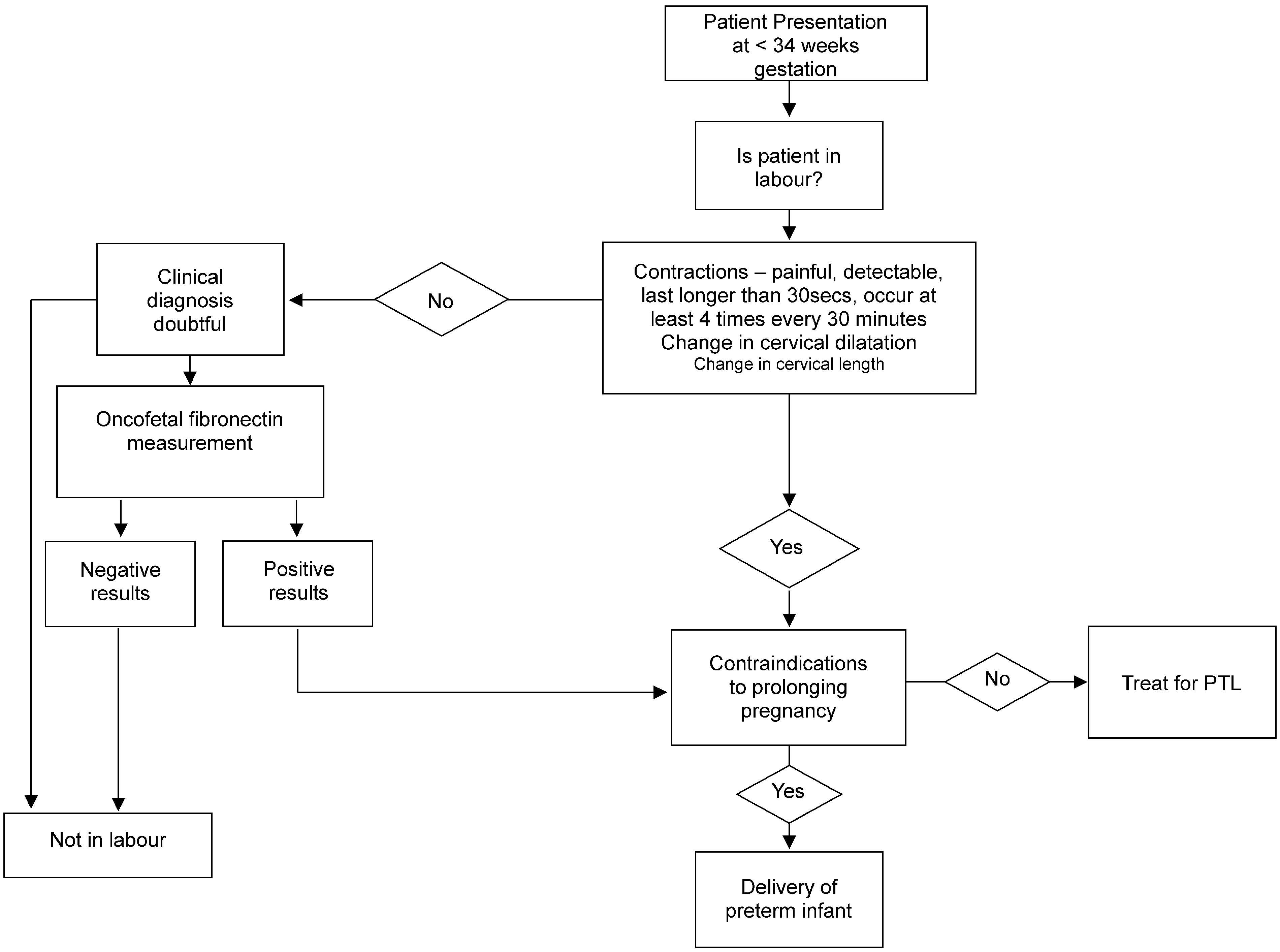
The diagnosis of spontaneous preterm labour
An algorithm describing the diagnosis of preterm labour is
On admission with suspected spontaneous preterm labour,
the accuracy of the expected date of confinement should bere-checked scrupulously because the best estimate willinfluence whether or not intervention should take place. If
the mother is sure of the last day of her last menstrual
period, had a regular monthly cycle and an early
These guidelines are based on the acute management of
ultrasound scan confirmed the date then menstrual dates
spontaneous preterm labour 5 34 weeks’ gestation. As a
should be used. If the dates are uncertain, or the cycle
consequence, the main management focus is centred on the
irregular, or there is a discrepancy of 4 10 days between
inhibition of preterm labour and therefore the administra-
the scan and the menstrual dates, then the scan dates
tion of tocolytics forms the majority of the recommenda-
tions obtained from the systematic literature review.
The diagnosis of spontaneous preterm labour on clinical
(1) contractions that are painful, palpable, last longer
than 30 seconds duration and occur at least four times every
The primary aims of tocolytic therapy are to delay delivery
to allow the administration of a complete course of
(2) there should be evidence of change in the position,
antepartum glucocorticoids in order to reduce the incidence
consistency, length and/or dilatation of the cervix.
and severity of idiopathic respiratory distress syndrome and
Where there is doubt using clinical parameters, then in
to arrange in-utero transfer to a centre with neonatal
centres where the technique is available, oncofetal fibro-
nectin may be considered in addition to clinical assessment.
The secondary aim of tocolytic therapy is to delay
Fetal fibronectin is an extracellular matrix glycoprotein
delivery to permit significant growth and maturity of the
produced by the chorion and concentrated in the amniotic
fetus and to reduce the perinatal mortality and morbidity
fluid. It is normally present in cervicovaginal secretions until
about 20 weeks and then disappears to reappear before the
Because some of the currently used tocolytic agents have
onset of labour at term. If the adhesive fibronectin interface
the potential to cause serious fetomaternal adverse effects,
between the chorion and the decidua is disturbed, fetal
informed consent from the patient, and/or partner should
fibronectin may reappear in the vaginal secretions at an
earlier gestation. As a result, the detection of fetalfibronectin in cervicovaginal secretion after 22 weeks’gestation has been proposed as an indicator of spontaneous
preterm labour (Lockwood et al., 1991).
agonists are related structurally to adrenalin and nora-drenalin and include such drugs as ritodrine, terbutaline,albuterol,
These b2-agonists act on receptors in the uterus to
increase cAMP in smooth muscle cells, which decreases
The systematic review produced six of 30 references that
intracellular free calcium and phosphorylation of myosin
studied the predictive value of fetal fibronectin and cervical
light chain kinase, which in turn inhibits myometrial
length for preterm delivery. The detection of fetal
contraction (Hearne and Nagey, 2000). Within 48 hours
Contractions — painful, detectable, last
Figure 1. Diagnosis of preterm labour (PTL) algorithm.
of administration, the b-agonists are able to reduce the
indirectly by stimulating the release of prostaglandins in
number of women who deliver preterm (King et al.,
decidual and fetal membranes, contributing further to
1998), but have not been found to produce a reduction
myometrial contractions and cervical ripening (Bossmar,
in perinatal mortality or morbidity (Rozenberg et al.,
Compared with b-agonists, in randomised double-blind
Several randomised clinical studies have shown the most
placebo-controlled trials atosiban (oxytocin antagonist,
widely used b-agonist, ritodrine, is equally as active as the
partial vasopressin antagonist) offers comparable effective-
calcium channel blocker, nifedipine, but with poorer
ness (i.e. the proportion of women remaining undelivered at
tolerability (Kupfermine et al., 1993; Papatsonis et al.,
48 hours and 7 days) as well as comparable efficacy and
1997; Garcia-Velasco and Gonzalez-Gonzalez, 1998; Koks
tolerability (non-delivery and no alternative tocolysis) at
et al., 1998; Al-Qattan et al., 2000; Papatsonis et al., 2000)
48 hours (European Atosiban Study Group, 2001) (Grade
A, Table II). Due to more favourable safety and tolerability
The maternal adverse events of b-agonists include
atosiban, assessed at 7 days, is significantly superior to b-
palpitations, tremor, nausea, vomiting, headache and
agonists. The likelihood of prolongation of pregnancy is
restlessness (RCOG, 1997). Pulmonary oedema occurs with
increased (Worldwide Atosiban versus Beta-agonists Study
an incidence of approximately one in 400 (Black et al., 1999;
Group, 2001) (Grade A, Table II). In addition, atosiban had
a significantly lower rate of cardiovascular side effects and a
The risk of these adverse events associated with b-
reduced need to discontinue therapy due to unacceptable
agonists in the management of spontaneous preterm labour
side effects. Significantly fewer patients required alternative
requires close monitoring of the mother in a high
tocolytic therapy following allocation to atosiban due to the
dependency unit. These have been addressed by the Royal
superior tolerability profile (Romero et al., 2000; Moutquin
College of Obstetrics and Gynaecology (RCOG, 1997) and
et al., 2000) (Grade A, Table II). Atosiban represents an
their recommendations for monitoring are shown in Table
advance in currently available tocolytics, and should be
considered a first-line tocolytic for the management ofspontaneous preterm labour (Worldwide Atosiban versusBeta-agonists Study Group, 2001) (Grade A, Table II).
Oxytocin is believed to initiate myometrial contractility by adirect effect on membrane-bound receptors that leads to an
Unlicensed tocolytic therapy: calcium channel
increase in intracellular calcium. It is also understood to act
Calcium channel blockers, such as nifedi-
International preterm labour council guidelines
Table II. Grade A evidence for the efficacy and tolerability of the b-agonists in comparison with other tocolytics. NB: in terms of efficacy, 4 implies a greater efficacy and in terms of tolerability, 4 implies a greater tolerability
Table III. The recommended guidelines for monitoring
fewer patients who have to discontinue treatment due to
IV administration with b-agonists produced by the
drug-associated side effects (Grade A). Since the Interna-
Guidelines from the Royal College of Obstetricians
Cochrane meta-analysis (King et al, 2003) also suggestedthat calcium antagonists (mainly nifedipine) were more
effective than other tocolytic agents (mainly b-agonists) in
terms of fewer births within 7 days of initiation of treatment
Maternal pulse and BP should be monitored every 15
and before 34 days’ gestation), with improvement in some
neonatal outcomes and a reduction in adverse maternal side
Chest auscultation should be performed every
effects (Grade A). Side effects commonly associated with
nifedipine include flushing, headache and rarely hypoten-
Strict input/output charts should be measured for
sion in the hypovolaemic patient (Childress and Katz,
Urea and electrolytes and haematocrit should be
Recent reviews of the evidence pertaining to the use of
nicardipine suggest that the safety profiles of these drugs are
Maternal blood glucose should be measured
incomplete and should lead to careful consideration before
use. It has been recommended that nicardipine should onlybe used in a clinical trial setting (King, 2001).
pine and nicardipine, inhibit the influx of calcium ionsinto myometrial cells, and the decreased intracellular
calcium results in decreased myometrial activity (Hearne
glandin synthetase inhibitors (e.g. indomethacin, sulindac
and ketorolac) decrease prostaglandin synthetase and
Calcium channel blockers, when compared with b-
block conversion of free arachidonic acid to prostaglan-
agonists, have a comparable tocolytic efficacy with a
din. As the prostaglandin E and F series are mediators of
reduction in neonatal morbidity (Papatsonis et al., 2001;
uterine contractions, a decrease in production results in
Tsatsaris and Carbonne, 2001) (Grade A, Table II).
decreased contractile activity (Hearne and Nagey, 2000).
As tocolytic agents calcium channel blockers, especially
Indomethacin is a potent inhibitor of prostaglandin
nifedipine, are more effective than b-agonists and there are
synthesis and has been used as a tocolytic agent since the
early 1970s. Indomethacin is effective in delaying preterm
infant (Grade A). They suggested that any further trials
labour and increases birth weight, results in shorter stays in
should be of high quality, large enough to assess serious
neonatal intensive care units and shorter intervals of
morbidity and mortality, compare different dose regimens
mechanical ventilation (Grades A or B, depending on study
and provide information about the neurodevelopmental
quoted) (Table IV). Conversely, contradictory evidence
shows that indomethacin fails to prolong gestation andinfants are delivered prematurely (Merrill et al., 1994)(Grade A).
In one study, indomethacin was associated with a
reduced risk of neonatal complications in infants born
Prolonging gestation with tocolytic therapy allows for the
between 24 and 31 weeks’ gestation (Gardner et al., 1996)
administration of antepartum glucocorticoids to reduce the
(Grade B). Morales and Madhav (1993) reported that
incidence and severity of respiratory distress syndrome and
indomethacin used to treat spontaneous preterm labour,
hence reduce neonatal morbidity and mortality. The
caused oligohydramnios and was associated with maternal
systematic literature review concentrated on those papers
side effects such as chest pain, shortness of breath, malaise
that studied the single and multiple administrations of
and pulmonary oedema (Grade A). Potential fetal adverse
effects include premature closure of the ductus arteriosus,
Ten of 63 references in the literature search provided
necrotising enterocolitis, respiratory distress syndrome and
Grade A evidence for the use of single rather than multiple
bronchopulmonary dysplasia (Highby and Suiter, 1999)
courses of antepartum glucocorticoids. The administration
of a single course of antepartum glucocorticoids to pregnantwomen, between 24 – 34 weeks’ gestation, at risk of pretermdelivery within 7 days, reduces the risk of death, respiratory
distress syndrome and intraventricular haemorrhage in the
magnesium sulphate is believed to be via competitive
preterm infant (Schmitz et al., 2000; Crowley 2001). This
antagonism to calcium for entry into myometrial cells.
has been reflected in the National Institutes of Health
Decreased intracellular free calcium results in decreased
Consensus Statement, 1994. The treatment should consist of
myometrial contractility (Hearne and Nagey, 2000).
two doses of 12 mg betamethasone given intramuscularly
In a study by Mittendorf et al. (1997), the Magnesium
24 hours apart or four doses of 6 mg dexamethasone given
and Neurologic Endpoints Trial (MagNET) showed that
magnesium sulphate was as effective, but no more effective
There is still debate about the use of repeated doses of
as a tocolytic agent than ritodrine, terbutaline, indometha-
antepartum glucocorticoids. Multiple doses of antepartum
cin or nifedipine (Grade A). This finding appears to reflect
glucocorticoids may be associated with early-onset neonatal
other evidence (see Table IV) that magnesium sulphate is
sepsis and death (Vermillion et al., 2000) (Grade B) or have
comparable to b-agonists and prostaglandin synthetase
no effect on these outcomes or others such as intraven-
inhibitors in prolonging gestation. The authors state that
tricular haemorrhage, bronchopulmonary dysplasia, necro-
safety and efficacy has not been demonstrated sufficiently
tising enterocolitis and birth weight (Aghajafari et al., 2001)
with magnesium sulphate. High doses (exceeding a total
(Grade B). A recent consensus panel (National Institutes of
dose of 48 g) have been associated significantly with
Health Consensus Development Panel, 2001) concluded
increased perinatal mortality (Scudiero et al., 2000) (Grade
that data from currently available studies assessing the
benefits and risks of the use of repeated courses of
Since the International Preterm Labour Council, the
antepartum glucocorticoids remains unanswered at this
Cochrane Database has also investigated the use of
Furthermore, there is evidence that delaying the use of
concluded that magnesium sulphate is ineffective at delaying
antepartum glucocorticoids in women with preterm prema-
birth or preventing preterm birth after preterm labour, and
ture rupture of the membranes (PPROM) may significantly
its use is associated with an increased mortality for the
increase the risk of fetomaternal infection (Crowley, 2001)
Table IV. Grade A and B evidence for the efficacy and tolerability for prostaglandin synthetase inhibitors andmagnesium sulphate in spontaneous preterm labour
Prostaglandin synthetase inhibitors and magnesium sulphate
International preterm labour council guidelines
(Grade A). At earlier gestation, the benefits may outweigh
The expected benefit in survival and reduced disability
the risks but at later gestations, the risk – benefit analysis
from prolonging gestation comes from three recent sources.
Magowan et al. (1999), showed that mortality fell from 80%at 24 weeks’ gestation to 10% at 30 weeks’ gestation andthat while 50% of preterm births occur after 35 weeks’
gestation, almost all the mortality occurs before this time
The Council agreed that the following investigations would
(Magowan et al., 1999). Secondly, between the gestational
ages of 23 and 27 weeks, neonatal survival increases in alinear fashion at a rate of 3% per day with a concomitant
(1) full blood count and group and save serum;
reduction in neonatal morbidity from 31% at 23 weeks to
(2) midstream specimen of urine examined for bacteruria;
7% at 27 weeks (Finnstro¨m et al., 1997). Thirdly, the
contribution of preterm birth to morbidity was highlighted
in the recently reported Epicure study (Costeloe et al.,
(4) low vaginal swab and rectal swab to be cultured in
2000). This study was designed to describe the survival and
selective broth medium for screening for Group B
health problems for all infants born before 26 weeks’
completed gestation in the United Kingdom and the
The role of infection in the aetiology of preterm labour and
Republic of Ireland. A total of 276 maternity hospitals
the implication this has on the choice of investigation on
provided information showing that 65% of these babies
admission will be the subject of a separate set of guidelines.
died in the delivery suite or in the neonatal intensive careunit, before discharge from hospital.
The most frequently cited cause of death was pulmonary
insufficiency. Data from the babies that survived showed
As soon as possible after the diagnosis of spontaneous
that failure to administer antenatal steroids and failure for
postnatal transfer for intensive care within 24 hours of birth
paediatricians involved in management decisions are
were predictive of major abnormalities based on cerebral
informed to ensure that a neonatal intensive care cot is
available on site or that in-utero transfer to a centre with
Follow-up data at 30 months from the Epicure study
showed that 49% of survivors had some form of disability
(mental and psychomotor development, neuromotor func-
Finnstro¨m et al. (1997) have shown that the level of care
tion, sensory and communication function) and nearly 50%
at birth and the level of subsequent neonatal care in the
of these met the criteria for severe disability using
neonatal intensive care unit are related directly to a lower
neurological and developmental assessment (Wood et al.,
rate of neonatal morbidity and mortality when compared
2000). Only 13% of infants survived to 30 months without
with babies born in hospitals without specialised staff and
equipment (Finnstro¨m et al., 1997) (Grade B). Hospitals
Absolute contraindications are those in which prolonga-
that had full resources for obstetric and neonatal intensive
tion of pregnancy is contraindicated per se, e.g. clinically
care had significantly lower infant mortality than those
apparent intrauterine infection, known lethal fetal congeni-
without. In-utero transfer is safer for the baby and
tal malformation, fulminating proteinuric pre-eclampsia
and any other urgent fetomaternal indication for delivery.
compared with neonatal transfer (Lamont et al., 1983)
Relative contraindications are those in which there is a
debate about the risks and benefits of intervention such as
If time permits, an ultrasound scan should be arranged to
antepartum haemorrhage, ruptured membranes, non-reas-
check for fetal viability, fetal morphology, fetal number,
suring fetal heart rate pattern on the cardiotocograph,
fetal presentation, placental site, an estimate of fetal weight
intrauterine growth restriction, insulin-dependent diabetes
and amniotic fluid volume index, all of which might affect
management. Appropriate analgesia following discussion
Tocolytics should not be used if there is a significant
with an anaesthetist should be arranged and opiates should
antepartum haemorrhage, especially if there are signs and
be avoided, if possible, to prevent central fetal and neonatal
symptoms of abruptio placentae. Following a mild bleed
due to placenta praevia, it is acceptable to use tocolytics
If intervention is contraindicated or unsuccessful, then
because they may help to stop uterine contraction and the
the mode of delivery of a preterm infant should be
stretch they induce, leading to further separation of the
individualised according to the gestational age, the fetal
presentation, the number of fetuses and the presence or
Tocolytics are rarely indicated after 32 weeks’ gestation
absence of non-reassuring fetal heart tracing on cardiotoco-
in the presence of ruptured membranes. At an earlier
graph. The debate with respect to the mode of delivery of
gestation, they may be administered when the risk – benefit
the preterm infant will be the subject of further Council
analysis is in favour of delaying delivery to allow a full
course of glucocorticoids to be administered or arrange-ments to transfer a woman to a centre with neonatalintensive care unit facilities.
Tocolytics to delay delivery of the preterm infant are
contraindicated where non-reassuring fetal heart rate
When considering intervention to prolong gestation, certain
patterns on the cardiotocograph occur in association with
absolute and relative contraindications should be consid-
a significant haemorrhage or with signs of fetomaternal
ered in order to minimise maternal and fetal morbidity and
infection or where the cardiotocograph trace is suggestive of
Severe intrauterine growth restriction may be associated
professionals such as neonatologists, genitourinary medi-
with congenital malformation, and consideration should be
cine physicians, microbiologists and geneticists together
given to this possibility before intervention. Severe placental
with basic scientists, such as molecular biologists, immunol-
insufficiency where continued intrauterine existence puts the
ogists, physiologists, biochemists and endocrinologists.
fetus at risk, is a contraindication to intervention although
It is hoped that, in time, these guidelines will be adopted
minor degrees of intrauterine growth restriction where
and adapted at a national level to be incorporated into
further fetal growth might be anticipated would not be a
clinical practice in local settings and to stimulate dialogue
contraindication to the use of a tocolytic. In cases where the
fetus is thought to be clinically or ultrasonographicallysmall for the dates, the calculation of the estimated date ofconfinement and the dates should be re-checked.
Well-controlled insulin-dependent diabetic women with
spontaneous preterm labour can safely be treated with
We are grateful to Healthcare Education Services Ltd for
tocolytics. Close monitoring is required because both
organising the meeting and for Wells Healthcare for assisting withthe manuscript. We are grateful to Ferring Pharmaceuticals who
glucocorticoids and particularly b-agonists are likely to
supported the meeting with an unrestricted educational grant.
affect diabetic control (Besinger and Lannucci, 1997; Fisheret al., 1997). Poorly controlled diabetes is a relativecontraindication to the use of b-agonist tocolytics andalternative tocolytics should be used where available.
Twins and higher-order births are associated with a
greater maternal plasma volume expansion (Cambell and
MacGillivray, 1997) and secondary hyperaldosteronism
Abramov Y., Nadjari M., Weinstein D., Ben-Shachar I.,
when compared with single pregnancies. Beta-agonists are
Plotkin V. and Ezra Y. (2000) Indomethacin for preterm
known to increase both aldosterone and renin levels in twin
labor: a randomised comparison of vaginal and rectal – oral
pregnancies (Lammintausta and Erkkola, 1979), which may
routes. Obstetrics and Gynecology, 95, 482 – 486.
potentiate the the risk of pulmonary oedema. Beta-agonists
Aghajafari F., Murphy K., Hannah M. and Amankwah K.
are therefore relatively contraindicated in multiple preg-
(2001) Repeated courses of antenatal corticosteroids: a
nancies, and alternative tocolytics should be used.
systematic review and meta-analysis. American Journal ofObstetrics and Gynecology, 184, S36.
Al-Qattan F., Omu A.E. and Labeeb N. (2000) A prospective
randomised study comparing nifedipine versus ritodrine for
the suppression of preterm labour. Medical Principles and
Preterm birth is the major cause of perinatal mortality and
morbidity in the developed world, although the manage-
Beall M.H., Edgar B.W., Paul R.H. and Smith-Wallace T.
ment of spontaneous preterm labour varies from unit to unit
(1985) A comparison of ritodrine, terbutaline and magnesium
and country to country. There is enough evidence based on
sulphate for the suppression of preterm labor. American
a systematic review to form a basis for consensus using
Journal of Obstetrics and Gynecology, 153, 854 – 859.
guidelines produced by a respected committee of experts in
Besinger R.E. and Iannucci T.A. (1997) Tocolytic therapy. In:
the field who manage spontaneous preterm labour on a
Preterm Labour, edited by Elder M.G., Lamont R.F. and
daily basis. However, it must be appreciated that definitions
Romero R., pp. 243 – 297. New York, Churchill Livingstone.
Bivins H.A., Newman R.B., Fyfe D.A., Campbell B.A. and
of spontaneous preterm labour and treatment protocols
Stramm S.L. (1993) Randomized trial of oral indomethacin
vary across clinical trials and therefore it is not always
and terbutaline sulfate for the long-term suppression of
possible to compare tocolytic treatment from one clinical
preterm labor. American Journal of Obstetrics and Gynecol-
trial with another. The International Preterm Labour
Council was set up with this in mind and with the hope
Black R.S., Lees C., Thompson C., Pickles A. and Campbell S.
that, with the development of preterm labour guidelines, it
(1999) Maternal and foetal cardiovascular effects of trans-
might contribute to a reduction in the fetomaternal
dermal glyceryl trinitrate and intravenous ritodrine. Obste-
mortality and morbidity associated with preterm birth.
trics and Gynecology, 94, 572 – 576.
The International Preterm Labour Council concluded
Bossmar T. (1998) Treatment of preterm labour with the
that every case of spontaneous preterm labour is a unique
oxytocin and vasopressin antagonist Atosiban. Journal ofPerinatal Medicine, 26, 458 – 465.
situation. The management of each patient has to be
Campbell D.M. and MacGillivray I. (1997) Maternal physio-
individualised in the light of the clinical circumstances and
logical responses and birthweight in singleton and twin
the full and informed consent of the pregnant mother and
pregnancies by parity. European Journal of Obstetrics,
Gynecology, and Reproductive Biology, 7, 17 – 24.
This being the case by necessity the guidelines, although
Chau A.C., Gabert H.A. and Miller J.M. (1992) A prospective
evidence-based, are generalised and follow a systematic
comparison of terbutaline and magnesium for tocolysis.
review that permits individualised variation within a
Obstetrics and Gynecology, 80, 847 – 851.
framework. This framework is not rigid, is open to
Childress C.H. and Katz V.L. (1994) Nifedipine and its
discussion and will change as new evidence becomes
indications in obstetrics and gynecology. Obstetrics and
Costeloe K., Hennessy E., Gibson A.T., Marlow N. and
As our understanding of the mechanism and aetiology of
Wilkinson A.R. (2000) The EPICure study: outcomes to
spontaneous preterm labour improves, and the remit of the
discharge from hospital for infants born at the threshold of
group expands to include the prediction and prevention of
viability. Pediatrics, 106, 659 – 671.
preterm birth and the role of infection and mode of delivery
Crowley P. (2001) Prophylactic Corticosteroids For preterm
of the preterm infant, further guidelines will be produced.
Birth [Cochrane Review]. The Cochrane Library, Issue 4.
These will require contributions from other health-care
International preterm labour council guidelines
Crowley P., Chalmers I. and Keirse M.J.N.C. (1990) The effects
King J.F., Flenady V.J., Papatsonis D.N.M., Dekker G.A.,
of corticosteroid administration before preterm delivery: an
Carbonne B. (2003) How to interpret and utilise the
overview from the evidence from controlled trials. British
Cochrane Review on calcium channel blockers for inhibiting
Journal of Obstetrics and Gynaecology, 97, 11 – 25.
preterm labour. Cochrane Database Systematic Reviews,
Crowther C.A., Hiller J.E., Doyle L.W. (2003) Magnesium
Issue 2, Oxford: Update Software Ltd.
Sulphate for Preventing Preterm Birth in Threatened Preterm
Koks C.A., Broelmann H.A., de Kleine M.J. and Manger P.A.
Labour [Cochrane Review]. The Cochrane Library, Issue 2,
(1998) A randomized comparison of nifedipine and ritodrine
for suppression of preterm labor. European Journal of
European Atosiban Study Group (2001) The oxytocin antago-
Obstetrics, Gynecology and Reproductive Biology, 77, 171 –
nist atosiban versus the b-agonist terbutaline in the treatment
of preterm labour. Acta Obstetrica et Gynecologica Scandi-
Kupfermine M., Lessing J.B., Yaron Y. and Peyser M.R.
(1993) Nifedipine versus ritodrine for suppression of preterm
Ferguson J.E., Dyson D.C., Schutz T. and Stevenson D.K.
labour. British Journal of Obstetrics and Gynaecology, 100,
(1990) A comparison of tocolysis with nifedipine or ritodrine:
analysis of efficacy and maternal, fetal and neonatal outcome.
Lammintausta R. and Erkkola R. (1979) Effect of long term
American Journal of Obstetrics and Gynecology, 163, 105 –
salbutamol treatment on renin aldosterone system in twin
pregnancy. Acta Obstetricia et Gynaecologica Scandinavica,
Finnstro¨m O., Otterblad Olausson P., Sedin G., Serenius F.,
Svenningsen N., Thiringer K., Tunell R., Wennergven M.
Lamont R.F. (2000) The pathophysiology of pulmonary
and Wesstrom C. (1997) The Swedish national prospective
oedema with the use of beta-agonists. British Journal of
study on extremely low birthweight (ELBW) infants.
Obstetrics and Gynaecology, 107, 439 – 444.
Incidence, mortality, morbidity and survival in relation to
Lamont R.F., Dunlop P.D., Crowley P., Levene M.I. and Elder
level of care. Acta Paediatrica, 86, 503 – 511.
M.G. (1983) Comparative mortality and morbidity of infants
Fisher J.E., Smith R.S., Lagrandeur R. and Lorenz R.P. (1997)
transferred in utero or postnatally. Journal of Perinatal
Gestational diabetes mellitus in women receiving beta-
adrenergics and corticosteroids for threatened preterm
Lees C.C., Lojacono A., Thompson C., Danti L., Black R.S.,
delivery. Obstetrics and Gynecology, 90, 880 – 883.
Tanzi P., White R. and Campbell S. (1999) Glyceryl trinitrate
French/Australian Atosiban Investigators Group (2001) Treat-
and ritodrine in tocolysis: an international multicenter
ment of preterm labor with the oxytocin antagonist atosiban:
randomised study. Obstetrics and Gynecology, 94, 403 – 408.
a double-blind, randomized, controlled comparison with
Lockwood C.J., Senyel A.E., Dische M.R., Casal D., Shah
salbutamol. European Journal of Obstetrics, Gynecology, and
K.D., Thung S.N., Jone S., Deligdisc L. and Garite J.J.
Reproductive Biology, 98, 177 – 185.
(1991) Foetal fibronectin in cervical and vaginal secretions as
Garcia-Velasco J.A. and Gonzalez-Gonzalez A. (1998) A
a predictor of preterm delivery. New England Journal of
prospective, randomised trial of nifedipine vs ritodrine in
threatened preterm labor. International Journal of Gynaecol-
Lopez-Bernal A. and TambyRaja R.L. (2000) Preterm labour.
ogy and Obstetrics, 61, 239 – 244.
Baillie`re’s Best Practice and Research. Clinical Obstetrics and
Gardner M.O., Owen J., Skelly S. and Hauth J.C. (1996)
Preterm delivery after indomethacin: a risk factor for
Magowan R.A., Pain M., Juszczak B.E. and McInnery K.
neonatal complications? Journal of Reproductive Medicine,
(1999) Neonates mortality among Scottish preterm singleton
births. Neonatal Intensive Care, 12, 47 – 50.
Hall M.H., Danielian P. and Lamont R.F (1997) The
Merrill J.D., Clyman R.I. and Norton M.E. (1994) Indometha-
importance of preterm birth. In: Preterm Labour, edited by
cin as a tocolytic agent: the controversy continues. Journal of
Elder M.G., Lamont R.F. and Romero R., pp. 1 – 28. New
Mittendorf R., Covert R., Boman J., Khoshnood B., Lee K.S.
Hearne A.E and Nagey D.A. (2000) Therapeutic agents in
and Siegler M. (1997) Is tocolytic magnesium sulphate
preterm labour: tocolytic agents. Clinical Obstetrics and
associated with increased total paediatric mortality? Lancet,
Highby K. and Suiter C.R. (1999) A risk – benefit assessment of
Morales W.J. and Madhav H. (1993) Efficacy and safety of
therapies for premature labour. Drug Safety, 21, 35 – 56.
indomethacin compared with magnesium sulphate in the
Hole J.W. and Tressler T.B. (2001) Management of preterm
management of preterm labour: a randomized study. Amer-
labour. Journal of American Osteopathic Association, 101,
ican Journal of Obstetrics and Gynecology, 169, 97 – 102.
Moutquin J.M., Sherman D., Cohen H., Mohide P.T.,
Jannet D., Abankwa A., Guyard B., Carbonne B., Marpeau L.
Hochner-Celnikier D., Fejgin M., Liston R.M., Dansgreau
and Milliez J. (1997) Nicardipine versus salbutamol in the
J., Mazor M., Shalev E., Boucher M., Glezerman M.,
treatment of premature labor. A prospective randomised
Zimmer E. and Rabinovici I.N. (2000) Double-blind,
study. European Journal of Obstetrics, Gynecology and
randomized, controlled trial of atosiban and ritodrine in
Reproductive Biology, 73, 11 – 16.
the treatment of preterm labour: a multicenter effectiveness
Keirse M.J.N.C. (1995) New perspectives for the effective
and safety study. American Journal of Obstetrics and
treatment of preterm labour. American Journal of Obstetrics
National Institutes of Health Consensus Development Panel
King J.F. (2001) Oral nicardipine was as efficacious as
(2001) Antenatal corticosteroids revisited; repeat courses.
magnesium sulfate for treatment of preterm labor, with
Obstetrics and Gynecology, 98, 144 – 150.
fewer side-effects. Evidence-based Obstetrics and Gynecology,
National Institutes of Health Consensus Statement (1994)
Effect of Corticosteroids for Foetal Maturation on Perinatal
King J.F., Grant A., Keirse M.J. and Chalmers I. (1998) Beta-
Outcome, Vol. 12, No. 2: 28 February – 2 March.
mimetics in preterm labour: an overview of the randomisedcontrolled trials. British Journal of Obstetrics and Gynaecol-ogy, 95, 211 – 222.
Papatsonis D.N., Van-Geijn H.P., Ader H.J., Lange F.M.,
Schorr S.J., Ascarelli M.H., Rust O.A., Ross E.L., Calfee E.L.,
Bleker O.P. and Dekker G.A. (1997) Nifedipine and ritodrine
Perry K.G. and Morrison J.C. (1998) A comparative study of
in the management of preterm labor: a randomised multi-
ketorolac (Toradol) and magnesium sulfate for arrest of
center trial. Obstetrics and Gynecology, 90, 230 – 234.
preterm labor. Southern Medical Journal, 91, 1028 – 1032.
Papatsonis D.N.M., Kok J.H., Van-Geijn H.P., Bleker O.P.,
Scudiero R., Khoshnood B., Pryde P.G., Lee K.S., Wall S. and
Ader H.J. and Dekker G.A. (2000) Neonatal effects of
Mittendorf R. (2000) Perinatal death and tocolytic magne-
nifedipine and ritodrine for preterm labor. Obstetrics and
sium sulphate. Obstetrics and Gynecology, 96, 178 – 182.
Sibony O., de Gayffier A. and Carbillon L, (1994) Has the use
Papatsonis D.N.M., Lok C.A.R., Bos J.M., Geijn H.P. and
of indomethacin during pregnancy consequences newborn
Dekker G.A. (2001) Calcium channel blockers in the
infants? Prospective study of 83 pregnant women and 115
management of preterm labour and hypertension in preg-
newborn infants. Archives de Pediatrie, 1, 709 – 715.
nancy. European Journal of Obstetrics, Gynecology, and
Spisso K.R., Harbert G.M. Jr and Thiagarajah S. (1982) The
Reproductive Biology, 97, 122 – 140.
use of magnesium sulfate as the primary tocolytic agent to
Romero R., Sibai B.M., Sanchez-Ramos L., Valenzuela G.J.,
prevent premature delivery. American Journal of Obstetrics
Veille J., Tabor B., Perry K.J., Varner M., Goodwin T.M.,
Lane R., Smith J., Shangold G. and Creasy G.W. (2000) An
Tsatsaris V., Carbonne B. (2001) Tocolysis with calcium
oxytocin receptor antagonist (atosiban) in the treatment of
channel blockers. Journal de Gyne´cologie Obste´trique et
preterm labour: a randomized, double-blind, placebo-con-
Biologie de la Reproduction (Paris), 30, 246 – 251.
trolled trial with tocolytic rescue. American Journal of
Vause S. and Johnston T. (2000) Management of preterm
Obstetrics and Gynecology, 182, 1173 – 1183.
labour. Archives of Disease in Childhood, Fetal and Neonatal
Royal College of Obstetricians and Gynaecologists (1997) Beta-
agonists for the care of women in preterm labour. Guideline
Vermillion S.T., Soper D.E. and Newman R.B. (2000)
Neonatal sepsis and death after multiple courses of antenatal
Rozenberg P. (2001) Tocolysis, use of beta-sympathomimetics
betamethasone therapy. American Journal of Obstetrics and
for threatening preterm delivery: a critical review. Journal de
Gyne´cologie Obste´trique et Biologie de la Reproduction
Wood N.S., Marlow M., Costeloe K., Gibson A.T. and
Wilkinson A.R. (2000) Neurologic and developmental dis-
Rozenberg P., Goffinet F. and Hessabi M. (1999) Comparison
ability after extremely preterm birth. New England Journal of
of the Bishop score, of sonographic measurement of the
cervical length and fibronectin determination in predicting
Woolf S.H., Grol R., Hutchinson A., Eccles M.P. and
time to delivery and the type of delivery at term. Bulletin de
Grimshaw J.M. (1999) The potential benefits, limitations
l’Academie Nationale de Medecine, 183, 589 – 599.
and harms of clinical guidelines. British Medical Journal, 318,
Rozenberg P., Goffinet F., Malagrida L., Giudicelli Y., Perdu
M., Houssin I. et al. (1997) Evaluating the risk of preterm
World Health Organization (1993) International Statistical
delivery: a comparison of foetal fibronectin and transvaginal
Classification of Diseases and Related Health Problems, 10th
ultrasonographic measurement of cervical length. American
revision, Vol. 2. Geneva, Switzerland: WHO.
Journal of Obstetrics and Gynecology, 176, 196 – 199.
Worldwide Atosiban versus Beta-agonists Study Group (2001)
Schmitz T., Goffinet F., Jarreau P.H., Moriette G. and Cabrol
Effectiveness and safety of the oxytocin antagonist atosiban
D. (2000) Repetition of corticoid treatment for foetal lung
versus beta-adrenergic agonists in the treatment of preterm
maturation: clinical and experimental scientific data. Journal
labour. British Journal of Obstetrics and Gynaecology, 108,
de Gyne´cologie Obste´trique et Biologie de la Reproduction
1.1. Introduction This general legal report deals with legal issues related to the taxation of fi-nancial undertakings within the Nordic countries. Because this report is based primarily on information presented in draft versions of the five national re-ports from the Nordic countries, some significant areas within the financial sector are not dealt with – the taxation of undertakings specif
Three of our classmates, John Shelby, Ed Garton, and Chuck Luton, have died of prostate cancer. It is not an easy death. In the cases of John and Ed, by the time a diagnosis was made, the cancer had already spread widely, and there was little that could be done other than ease the inevitable. They were both gone within months of the diagnosis. Bill Bailey forwarded this note from Chuck Luton on D
 Contractions — painful, detectable, last
Figure 1. Diagnosis of preterm labour (PTL) algorithm.
Contractions — painful, detectable, last
Figure 1. Diagnosis of preterm labour (PTL) algorithm.