Tadalafil zeigt eine konstante Resorption im Gastrointestinaltrakt, mit maximalen Plasmaspiegeln nach rund zwei Stunden. Der Wirkstoff verteilt sich gut im Gewebe und weist eine hohe Plasmaproteinbindung auf. Seine lange Halbwertszeit erlaubt eine verlängerte Wirkphase. Der Metabolismus erfolgt über das hepatische Enzymsystem CYP3A4, mit der Bildung inaktiver Metaboliten. Exkretion geschieht primär über den Stuhl. Die Häufigkeit von Nebenwirkungen steigt mit der Dosis, wobei vor allem vasodilatatorische Effekte dominieren. Ein gängiger Bezugspunkt in pharmakologischen Analysen ist cialis ohne rezept, das mit dieser Wirkstoffklasse assoziiert ist.
Aspartame: scientific evaluation in the postmarketing period
Regulatory Toxicology and Pharmacology 34, 221–233 (2001) doi:10.1006/rtph.2001.1500, available online at http://www.idealibrary.com on
Aspartame: Scientific Evaluation in the Postmarketing Period
Harriett H. Butchko∗ and W. Wayne Stargel†
∗Medical and Scientific Affairs and †Research and Development, The NutraSweet Company, Mt. Prospect, Illinois 60056
Received March 14, 2001; published online November 20, 2001
methanol. These components are utilized by the body in
Prior to marketing, the safety of the high-intensity
the same way as when they are also derived from foods,
sweetener aspartame for its intended uses as a sweet-
such as meat, milk, fruits, and vegetables (Ranney et al.,
ener and flavor enhancer was demonstrated by the results of over 100 scientific studies in animals and
Further, the components of aspartame are derived
humans. In the postmarketing period, the safety of
in much larger amounts from these common foods. aspartame was further evaluated through extensive
For example, a glass of milk provides about 6 times
monitoring of intake, postmarketing surveillance of
more phenylalanine and 13 times more aspartic acid
anecdotal reports of alleged health effects, and addi-
and a glass of tomato juice provides about 6 times
tional research to evaluate these anecdotal reports and
more methanol than an equivalent volume of bever-
other scientific issues. The results of the extensive in-
age sweetened 100% with aspartame (Butchko and
take evaluation in the United States, which was done
Kotsonis, 1989, 1991). Thus, much of the scientific re-
over an 8-year period, and the results of studies done
search, both before and after regulatory approval, fo-
in other countries demonstrated intakes which were
cused on the safety of these components. well below the acceptable daily intakes set by the FDA
Prior to marketing, aspartame underwent intensive
and regulatory bodies in other countries, as well as the
scientific scrutiny and regulatory review. Extensive tox-
Joint FAO/ WHO Expert Committee on Food Additives.
icologic and pharmacologic research was done in labo-
Evaluation of the anecdotal reports of adverse health effects, the first such system for a food additive, re-
ratory animals using much greater doses of aspartame
vealed that the reported effects were generally mild
than people would possibly ingest (Aspinall et al., 1980;
and also common in the general population and that
Bianchi et al., 1980; Lennon et al., 1980; Potts et al.,
there was no consistent or unique pattern of symptoms
1980; Saunders et al., 1980; Molinary, 1984; Kotsonis
that could be causally linked to consumption of aspar-
and Hjelle, 1996). From the results of the toxicology
tame. Finally, the results of the extensive scientific re-
studies, a no-observed-effect level (NOEL) of greater
search done to evaluate these allegations did not show
than 2000–4000 mg/kg body wt was established for as-
a causal relationship between aspartame and adverse
partame. The animal toxicology data were used by the
effects. Thus, the weight of scientific evidence confirms
Scientific Committee for Food (1985) of the European
that, even in amounts many times what people typi-
Economic Communities, the Joint FAO/ WHO Expert
cally consume, aspartame is safe for its intended uses
Committee on Food Additives (JECFA, 1980), and the
as a sweetener and flavor enhancer. C 2001 Elsevier Science
Canadian HPB (Health and Welfare Canada, 1979) to
Key Words: aspartame; postmarketing surveillance;
establish an acceptable daily intake (ADI) of 40 mg/kg
intake; acceptable daily intake; ADI; anecdotal reports;
body wt for aspartame. When aspartame was first ap-
safety; review.
proved in the United States in 1974, the FDA autho-rized an ADI of 20 mg/kg body wt for aspartame (FDA,1974). The ADI is the amount of an additive, which if
INTRODUCTION
consumed daily over a lifetime, would be considered safeand is usually 1% of the NOEL (Lu, 1988; Renwick,
Also prior to approval, the safety of aspartame and
phenylalanine methyl ester) has been consumed in
its metabolic constituents was assessed in humans in
more than 6000 products by hundreds of millions of
several subgroups: healthy infants, children, adoles-
people in countries around the world. Aspartame is
cents, and adults, obese individuals, diabetics, lactating
unique among high-intensity sweeteners because it is
women, and individuals heterozygous for the genetic
metabolized by digestive esterases and peptidases to
disease phenylketonuria (PKU) who have a decreased
three common dietary components—the amino acids,
ability to metabolize the essential amino acid pheny-
aspartic acid and phenylalanine, and a small amount of
lalanine. These and longer-term studies showed no
C 2001 Elsevier Science
very small number of consumers in the 99th percentile
(Hoffman, 1972, 1973; Langlois, 1972; Frey, 1973,
may have large and variable intakes, which may skew
1976; Knopp et al., 1976; Koch et al., 1976; Stern et al.,
the data markedly. Thus, the FDA now uses projections
1976; Stegink et al., 1977, 1979a,b, 1980, 1981a,b,
at the 90th percentile as the benchmark of high-level
1983; Filer et al., 1983). The results of the human
consumers. The more conservative 97.5th percentile is
studies, along with the animal research, provided con-
used in the United Kingdom (MAFF, 1990).
vincing evidence that aspartame was safe for generaluse, including by pregnant women and children. The
Aspartame Intake in the United States
FDA responded to these additional data by increasing
Actual aspartame consumption was tracked in the
the ADI for aspartame to 50 mg/kg body wt in 1983
United States by MRCA Information Services (North-
(FDA, 1984). The ADI for aspartame is the sweetness
brook, IL) (Abrams, 1986, 1992; Butchko and Kotsonis,
equivalent of a 60 kg person consuming approximately
1991, 1994, 1996; Butchko et al., 1994) from 1984 to
600 grams (1.3 pounds) of sugar daily over a lifetime,
1992 through detailed menu census surveys from over
an amount well above consumption patterns for sugar.
2000 households a year. During the 14-day survey, all
In order to inform individuals with homozygous PKU,
foods eaten both at home and away from home were
who cannot properly metabolize phenylalanine, the
U.S. FDA and other regulatory agencies require a label
Because of their smaller body weights, children may
statement on products with aspartame to indicate that
consume more of an additive on a milligram per kilo-
gram basis than adults. To evaluate intake by children
Since approval, aspartame has undergone further in-
specifically, data also were recorded by age group: 0–
vestigation through postmarketing surveillance and re-
23 months, 2–5 years, 6–12 years, 13–17 years, and
search to evaluate various scientific issues. Research
18 years and over, as well as all age groups together. In
was done to evaluate aspartame intake levels relative to
addition, intakes by special population subgroups such
the ADI, as was extensive postmarketing surveillance
as diabetics and people on weight-reduction programs,
of anecdotal reports of adverse health effects, the first
who might be enthusiastic users of aspartame with po-
such program for a food additive. In addition, several
tentially higher intakes, and women of childbearing po-
potential health issues, e.g., whether aspartame has an
tential and pregnant women were also monitored.
effect on headaches, allergies, seizures, behavior, cog-
Because of its intense sweetness, only small amounts
nitive function, etc., were evaluated through additional
of aspartame are needed to sweeten foods (see Table 1).
studies. The continued scientific evaluation of aspar-
Thus, it would be expected that intake of aspartame
tame in the postmarketing period is discussed in this
would be low. The MRCA survey demonstrated that
the average intake over the 14-day period for the gen-eral population of aspartame “eaters” (at the 90th per-
POSTMARKETING SURVEILLANCE: EVALUATION
centile) ranged from 1.6 to 3.0 mg/kg/day. As shown
OF ASPARTAME INTAKE
in Table 2, intake of aspartame at the 90th percentile,even by children, diabetics, people on weight-reduction
As part of the safety evaluation for a food additive,
diets, and females of childbearing age, was only approx-
regulators evaluate projected use levels relative to the
imately 5–10% of the ADI in the United States.
ADI. If projected intake levels approach or exceed the
Data from other types of consumption evaluations
ADI, restrictions may be imposed, such as limiting ap-
in the United States corroborate these results. Upon
provals for some categories of use to decrease potential
analysis of 1-day diary data from the U.S. Depart-
ment of Agriculture (USDA) Continuing Survey of Food
Before approval, projected average intake levels
of aspartame in the United States ranged from8.3 mg/kg/day, if all sucrose in an average-sized per-
son’s diet was replaced by aspartame, to 25 mg/kg/day
Approximate Aspartame Content of Some
if all dietary carbohydrate could be replaced by aspar-
Common Foods
tame. Based on dietary records from about 12,000 indi-viduals, it was estimated that, if all possible foods were
replaced with aspartame-containing foods, the 99th
percentile daily consumption of aspartame would be34 mg/kg (FDA, 1981).
At the time of approval of aspartame, the FDA consid-
ered the 99th percentile estimated intake as represen-
tative of high-level consumers. Since that time, the FDA
has determined that the 99th percentile is unduly con-
servative and probably unrealistic (FDA, 1986), as the
SCIENTIFIC EVALUATION OF ASPARTAME IN THE POSTMARKETING PERIOD
Aspartame Intake (mg/kg/day) in the General Population and Various Subpopulations in the United States (90th Percentile, “Eaters” Only, 14-Day Average)
Intakes by Individuals (CSFII) from over 1500 women,
France. From 1991 to 1992, aspartame intake was
aspartame intake ranged from 0 to 16.6 mg/kg/day; over
0.6 and 1.0 mg/kg/day at the 90th and 95th percentiles,
90% of the women who reported aspartame consump-
respectively (Chambolle et al., 1994). A limitation of the
tion had intakes less than 5 mg/kg/day (Heybach and
study was that data for some categories were missing,
Smith, 1988). Although per capita disappearance data
and there were no data for food consumed outside the
may underestimate consumption since both eaters and
home. In a more recent study, intake of aspartame was
“noneaters” are included, aspartame consumption for
evaluated in insulin-dependent diabetic children ages
the total population (based on a 50-kg person) can be es-
2–20 years (Garnier-Sagne et al., 1997) using a 5-day
timated to be about 1.6 mg/kg/day based on USDA per
diary questionnaire. Intake by aspartame consumers
capita disappearance data (Heybach and Allen, 1988).
at the mean, 97.5th percentile and maximum, were2.4, 7.8, and 15.6 mg/kg/day, respectively. All sugar-free
Aspartame Intake in Other Countries
products were assumed to contain only one sweetener atits maximum authorized level; thus, estimations were
The results of surveys from 10 other countries have
found intake levels of aspartame to be remarkably con-sistent with those in the United States, and all are well
Germany. In 1988–1989, consumption of the sweet-
eners aspartame, cyclamate, and saccharin was eval-uated in Germany. The 90th percentile average daily
Australia. In 1994, mean consumption levels of as-
intake for aspartame consumers was 2.75 mg/kg/day
partame were 6 and 7% of the ADI for all respondents
to a 7-day survey and total consumers, respectively. The90th percentile consumption was 23% of the ADI; how-
Italy. Average aspartame intake among Italian
ever, the small sample made a precise estimate of 90th
teenagers who were known to be users of diet products
percentile intake difficult (National Food Authority,
was estimated to be only 0.03 mg/kg/day; the maximum
aspartame intake was 0.39 mg/kg/day (Leclercq et al.,1999). Brazil. Median aspartame intake by the users of
intense sweeteners was 2.9% of the ADI; median in-
Netherlands. Based on food frequency question-
takes by diabetics and individuals on weight-control
naires, mean aspartame intake was estimated to
regimens were 1.02 mg/kg/day (2.6% of the ADI) and
be 2.4 mg/kg/day, with a 95th percentile intake of
1.28 mg/kg/day (3.2% of the ADI), respectively (Toledo
7.5 mg/kg/day. Using food intake records, mean intake
was 1.9 mg/kg/day while 95th percentile intake was5.2 mg/kg/day (Hulshof and Bouman, 1995). Canada. In 1987, the general population of aspar-
tame eaters in Canada consumed 5.5 mg/kg/day dur-
Norway. The average estimated intake of aspartame
ing cold weather months and 5.9 mg/kg/day during
varied from 0.9 to 3.4 mg/kg/day among males and fe-
warm weather months (7-day average, 90th percentile)
males and various age groups (Bergsten, 1993). United Kingdom. In the United Kingdom in 1988,
Finland. Nearly three-quarters (73%) of the diabetic
aspartame consumption (90th percentile) was 4% of the
children surveyed in Finland consumed aspartame-
ADI or about 1.6 mg/kg/day. Children and diabetics in-
containing products, with a mean intake of 1.15 mg/
gested only 7 and 6%, respectively, of the ADI at the
kg/day, less than 3% of the ADI (Virtanen et al., 1988).
90th percentile (Hinson and Nicol, 1992). From another
survey (MAFF, 1990), median and maximum aspar-
FDA to request the Centers for Disease Control (CDC)
tame intakes were 1.0 and 1.60 mg/kg/day, respectively,
to evaluate these reports (Centers for Disease Control,
in 2- to 5-year-old children and 0.25 and 6.20 mg/kg/day,
1984; Bradstock et al., 1986). In 1985, the FDA’s Center
respectively, in 35- to 64-year-old adults. For the general
for Food Safety and Applied Nutrition (CFSAN) started
population, median, maximum, and 97.5th percentile
its own process, the Adverse Reaction Monitoring Sys-
intakes were 16, 372, and 109 mg, respectively. For a
tem (ARMS), to monitor accounts of health problems
60-kg person, these are equal to 0.3, 6.2, and 1.8 mg/
anecdotally associated with consumption of foods, food
and color additives, and vitamin/mineral supplements
In 1994, the 97.5th percentile of aspartame con-
(Tollefson, 1988; Tollefson et al., 1988).
sumption in diabetics was found to be 10.1 mg/kg/day,only about 25% of the ADI, even among individuals
Centers for Disease Control Evaluation
who would likely be frequent consumers of aspartame
More than 500 reports were analyzed by the CDC,
and almost half underwent detailed follow-up and eval-uation. Most complainants were white women aged
21–60 years, randomly distributed throughout the
Actual intake levels of aspartame were monitored
United States with one exception. Aspartame had been
from 1984 to 1992 through dietary surveys in the
subjected to substantial negative media coverage in
United States. Average daily aspartame intake at the
Arizona, prompting proportionately more reports from
90th percentile (eaters only) in the general popula-
that state. While reports were received about a vari-
tion ranged from about 2 to 3 mg/kg body wt. Con-
ety of different symptoms, two-thirds fell into the neu-
sumption by 2- to 5-year-old children in these surveys
rologic/behavioral category. These consisted mostly of
ranged from about 2.5 to 5 mg/kg/day. Aspartame in-
headache, mood alterations, insomnia, and dizziness.
take has also been estimated in several other countries.
About a quarter of the reports were gastrointestinal,
Although survey methodologies differed among these
including abdominal pain, nausea, diarrhea, and vomit-
evaluations, aspartame intake is remarkably consistent
ing (Centers for Disease Control, 1984; Bradstock et al.,
across studies and is well below the ADI.
The CDC reported that “Despite great variety over-
all, the majority of frequently reported symptoms were
POSTMARKETING SURVEILLANCE: EVALUATION
mild and are symptoms that are common in the gen-
OF ANECDOTAL REPORTS OF HEALTH EFFECTS
eral populace” (Centers for Disease Control, 1984). Nospecific clinical syndromes that suggest a causal rela-
In the 1940s and 1950s, when many new drugs were
tionship with aspartame were observed. The CDC con-
being developed and marketed, it was realized that the
cluded that focused clinical studies would be the best
full spectrum of adverse reactions was not always ap-
way to address thoroughly the issues raised by the anec-
parent until a drug had been used by many patients
dotal reports (see Beyond Postmarketing Surveillance).
over time (Faich, 1986). It was concluded that, alongwith extensive preapproval studies, a postmarketing
surveillance system was needed to document and evalu-ate spontaneous reports of adverse reactions associated
Unlike the case of pharmaceuticals, where most infor-
mation is received from physicians, information regard-
Shortly after aspartame’s widespread marketing,
ing food additives is largely obtained from consumers.
there were a number of anecdotal reports of health ef-
In the case of aspartame, about 70% of the reports in
fects, which some consumers related to their consump-
ARMS were provided by The NutraSweet Company. Re-
tion of aspartame-containing products. Not unexpect-
ports to ARMS are categorized based on the severity of
edly, negative media stories influenced the numbers
symptoms and on the basis of the consistency and fre-
and types of these reports. The NutraSweet Company
quency with which they occur. Any reports of a serious
developed a postmarketing surveillance system for as-
nature are investigated by FDA field inspectors through
partame, based on the principles used for postmar-
interviews and medical record review.
keting surveillance of pharmaceuticals, to document
Based upon its review, the FDA concluded that there
and evaluate these anecdotal reports (Butchko and
is no “reasonable evidence of possible public health
Kotsonis, 1994; Butchko et al., 1994, 1996). Data from
harm” and “no consistent or unique patterns of symp-
this system were evaluated by the company and also
toms reported with respect to aspartame that can be
shared with the U.S. FDA, as discussed below.
causally linked to its use” (Tollefson, 1988; Tollefson
Following the approval of aspartame in carbonated
beverages in 1983, an increase in the reporting of
In a 1995 FDA report on aspartame (FDA, 1995),
adverse health events allegedly associated with the
a total of 7232 consumer reports had been received
consumption of aspartame-containing products led the
since marketing; only 11% were classified as serious.
SCIENTIFIC EVALUATION OF ASPARTAME IN THE POSTMARKETING PERIOD
Headache topped the list of symptoms reported,
mid-1980s had a significant impact on the number of
followed by dizziness, mood changes, and nausea/
anecdotal reports. As seen in Fig. 1, the number of re-
vomiting. The report noted the decline, since the peak in
ports increased markedly during that time and, as the
1985, of reports from consumers regarding aspartame
controversy decreased in the late 1980s and early 1990s,
and further stated, “In summary, the number of adverse
reaction complaints received by the FDA and the nature
As there are more than 100 million aspartame users
of these reports in terms of demographic distribution,
in the United States, it is inevitable that some of them
severity, strength of association with the product, and
will experience medical ailments temporally associated
symptoms remain comparable to those from previous
with consumption of an aspartame-containing product
simply by chance. A temporal association does not mean
FDA also separately analyzed the 251 reports of
a causal association. The error of associating causal-
seizure anecdotally associated with aspartame con-
ity to coincidence is perhaps best stated by one scien-
sumption received through ARMS from 1986 to 1990
tist who stated, “As aspartame is estimated to be con-
and concluded that almost half were highly unlikely to
sumed by about half the U.S. population, one need not
be related to aspartame (Tollefson and Barnard, 1992).
be an epidemiologist to grasp the problem of establish-
Furthermore, the FDA could not exclude the possi-
ing a cause-and-effect relationship. Half the headaches
bility that the remaining reports had not simply oc-
in America would be expected to occur in aspartame
curred by chance. FDA concluded that the anecdotal re-
users, as would half the seizures and half the purchases
ports “did not support the claim that the occurrences of
the seizures were linked to consumption of aspartame”(Tollefson and Barnard, 1992). It was further concluded
that the data did not suggest the need for a controlled
The postmarketing surveillance of reports of adverse
clinical study to evaluate this issue.
health effects allegedly associated with aspartame wasthe first such evaluation for a food additive. Extensive
The NutraSweet Company System for Health
monitoring and evaluation of these reports over many
years led to the conclusion that the reported symptoms
The NutraSweet Company’s postmarketing surveil-
generally were mild and common in the general popu-
lance system, which continued for 12 years after mar-
lation. There was no evidence to suggest a causal re-
keting in the United States, was a collaborative ef-
lationship with aspartame; however, “focused” clinical
fort between the Consumer Center, where the staff
studies would be the best way to address thoroughly the
was responsible for data collection, documentation, and
issues raised by the anecdotal reports.
follow-up, and the Clinical Research Group, wherephysicians provided medical expertise for evaluation ofthe reports. As noted in the CDC and FDA reports dis-
BEYOND POSTMARKETING SURVEILLANCE
cussed above, symptoms allegedly associated with as-
Research to Evaluate Allegations of Health Effects
partame tended to be mild and were also common inthe general population.
A number of studies, including focused clinical stud-
Not unexpectedly, the negative media stories and re-
ies in humans, were done to address scientific issues,
sulting controversy about aspartame in the early to
including the anecdotal reports of alleged health effects
Reports of health effects anecdotally associated with aspartame 1982–1994.
associated with aspartame. A long-term clinical study
serum ratio of phenylalanine to the other large amino
using high doses of aspartame (75 mg/kg/day for 24
acids (Phe/LNAA), thereby selectively increasing brain
weeks or about 25–30 times current consumption levels
phenylalanine concentrations. It was further hypothe-
at the 90th percentile) resulted in no significant differ-
sized that such increased entry of phenylalanine into
ences in clinical or biochemical parameters or adverse
the brain may result in disturbances in monoaminergic
experiences compared with a placebo (Leon et al., 1989).
Focused clinical studies evaluated whether aspartame
However, review of the numerous studies in labo-
causes headache, seizures, or allergic-type reactions in
ratory animals evaluating whether aspartame has an
individuals who firmly believed that aspartame caused
effect on various brain neurotransmitter systems has
shown no consistent effects of enormous amounts ofaspartame (Schomer et al., 1996). In addition, the re-
Headaches. Koehler and Glaros (1988) reported the
sults of additional animal studies demonstrated that
results of an outpatient study to evaluate the effect of
increases in brain phenylalanine concentrations af-
aspartame on the occurrence of migraine headache in
ter enormous doses of aspartame do not affect brain
migraineurs and concluded that aspartame caused a
monoaminergic neurotransmission (Garattini et al.,
significant increase in the frequency of headaches but
1988; Perego et al., 1988; Reilly et al., 1989, 1990).
not in the intensity or duration of headaches. This study
Furthermore, any effect that aspartame may have on
was criticized (Amery, 1988; Schiffman, 1988) because
the selective entry of phenylalanine into the brain is
of several statistical issues that made it difficult to draw
not unique to aspartame. For example, consumption
any valid conclusions from this study; data from only 11
of equisweet amounts of sugar has similar effects on
of the 25 subjects were reported, and the effects on fre-
the Phe/LNAA, through insulin-mediated changes in
quency of headaches can be attributed largely to data
the serum concentrations of these amino acids (Martin-
from only 2–3 subjects. From another outpatient study,
Du Pan et al., 1982; Stegink et al., 1987; Wolf-Novak
Van Den Eeden et al. (1994) reported that subjects had
et al., 1990; Burns et al., 1991).
more days with headaches, but there was no difference
Furthermore, numerous studies in humans have
in the length or intensity of headaches. This study was
demonstrated that even massive doses of aspartame,
criticized (Levy et al., 1995; Schiffman, 1995) because
many times those typically consumed, have no effect on
the results from one subject of the 32 enrolled largely
cognitive performance, mood, or behavior compared to
accounted for any difference between aspartame and
a placebo (Wolraich et al., 1985, 1994; Ferguson et al.,
placebo. When individuals who were convinced that as-
1986; Goldman et al., 1986; Milich and Pelham, 1986;
partame had caused their headaches were evaluated in
Kruesi et al., 1987; Ryan-Harshman et al., 1987; Lieber-
a randomized, double-blind, placebo-controlled study in
man et al., 1988; Dodge et al., 1990; Lapierre et al., 1990;
the controlled environment of a Clinical Research Unit
Saravis et al., 1990; Stokes et al., 1991, 1994; Shaywitz
at Duke University, aspartame (at a dose about 10 times
et al., 1994a; Trefz et al., 1994; Spiers et al., 1998). These
90th percentile consumption) was no more likely than
studies were done in both healthy children and adults,
a placebo to elicit headache (Schiffman et al., 1987).
including college students and pilots, as well as in sub-
Allergenicity. Early on, Kulczycki (1986) reported a
populations who were thought to be possibly “more sen-
single case report of an individual he believed was al-
sitive,” such as children with attention deficit disorder
lergic to aspartame. Geha and co-workers (1993) later
and adults who are heterozygous for phenylketonuria
reported the results of a multicenter, randomized,
(PKUH). Various assessments of mood, behavior, and
double-blind, placebo-controlled, crossover study done
cognitive performance were utilized in these studies.
with individuals who were convinced they were allergic
For example, in the study in PKUH, a computerized
to aspartame. These investigators concluded that as-
battery of tests that had been shown to detect sub-
partame and its conversion products are no more likely
tle changes in cognitive performance not detected by
than a placebo to cause allergic-type reactions. Another
conventional tests, and computerized, spectral analysis
study also demonstrated that alleged allergic-type reac-
of the electroencephalograms were used (Trefz et al.,
tions to aspartame were not reproducible under blinded
conditions (Garriga et al., 1991).
From a study in depressed patients, Walton et al.
(1993) concluded that aspartame increased the fre-
Brain function: Neurotransmission, cognition, behav-
quency and severity of adverse experiences in these
ior, mood, and seizures. A number of the aspartame al-
individuals. The study was designed to include 40 de-
legations centered on various aspects of brain function.
pressed subjects and 40 nondepressed subjects. How-
The underlying hypothesis was that aspartame, as a
ever, only 13 subjects (8 with depression and 5 without
source of phenylalanine without the other large neutral
depression) were enrolled before the study was stopped,
amino acids (i.e., tryptophan, valine, leucine, isoleucine,
and only 11 completed the study. This study has been
methionine, histidine) which compete for transport
criticized (Butchko, 1994; Schomer et al., 1996) because
across the blood–brain barrier, would increase the
the authors apparently combined unrelated adverse
SCIENTIFIC EVALUATION OF ASPARTAME IN THE POSTMARKETING PERIOD
complaints to show a statistically significant result,as there were no differences between aspartame andplacebo in specific types of complaints.
Numerous studies were done in various animal mod-
els of epilepsy ranging from studies in both epileptic andnonepileptic rats, mice, and epileptic baboons. Enor-mous doses of aspartame or phenylalanine (in the rangeof thousands of mg/kg body wt) were used in thesestudies. From the results, there is compelling evidencethat aspartame is not a proconvulsant (Guiso et al.,1988, 1991; Pinto and Maher, 1988; Cain et al., 1989;Dailey et al., 1989, 1991; Fisher, 1989; Meldrum et al.,1989; Sze, 1989; Tilson et al., 1989; Zhi and Levy, 1989;Diomede et al., 1991; Jobe et al., 1992; Jobe and Dailey,1993; Lajtha et al., 1994; Sperber et al., 1995; Helaliet al., 1996).
From a study in children with absence seizures,
Intake of aspartic acid from the normal diet compared to
Camfield and co-workers (1992) reported that aspar-
that from aspartame (90th percentile, 14-day average, “eaters” only)in adults and 4-year-old children.
tame compared to sugar may increase the amountof EEG spike-wave activity. However, according toShaywitz and Novotny (1993), sugar is not a true
tame’s phenylalanine content are those with phenylke-
“placebo” as it may affect the EEG and thus may have
tonuria, a rare genetic disease in which the body can-
confounded the results. Further, the baseline period of
not properly metabolize phenylalanine. These individ-
the study was too short to have been able to deter-
uals must severely restrict phenylalanine intake from
mine reliably if aspartame had an effect. Rowan et al.
all dietary sources, including aspartame.
(1995) reported the results of a randomized, double-
Methanol. Aspartame yields approximately 10%
blind, placebo-controlled, crossover study with 5 contin-
methanol by weight. The amount of methanol released
uous days of EEG monitoring in a clinical research unit
from aspartame is well below normal dietary exposure
with individuals who were convinced that aspartame
to methanol from fruits, vegetables, and juices (Butchko
caused their seizures. With doses of aspartame about
and Kotsonis, 1989, 1991). Aspartame, even in amounts
17 times 90th percentile consumption, there was no evi-
many times those consumed from products, does not
dence of aspartame-activated epileptiform activity, and
significantly change baseline blood concentrations of
aspartame was no more likely than placebo to cause
methanol or formate (Stegink et al., 1981a, 1983).
seizures. Shaywitz et al. (1994b) reported the results of
Whereas methanol exposure at the 90th percentile
a 4-week study in children with seizure disorders, in-
of chronic aspartame consumption is 0.3 mg/kg/day,
cluding absence seizures. After a dose about 10 times
the FDA has established acceptable levels of expo-
90th percentile intake levels, aspartame neither pro-
sure to methanol at 7.1 to 8.4 mg/kg/day for 60 kg
voked nor exacerbated seizures nor altered EEG activ-ity compared to placebo.
That aspartame does not affect brain function is not
surprising considering that consumption of aspartame-sweetened foods does not increase plasma phenylala-nine concentrations beyond those which normally oc-cur postprandially (Stegink et al., 1977, 1979a, 1980). For example, doses of aspartame of approximately30 mg/kg/day (about 10 times 90th percentile daily in-take) do not increase plasma phenylalanine concen-trations above those observed after eating a protein-containing meal in normal adults, phenylketonuricheterozygotes, or non-insulin-dependent diabetic pop-ulations (Filer and Stegink, 1989).
Further, at current levels of consumption, only a
small fraction of daily dietary intake of aspartic acidand the essential amino acid phenylalanine by adultsand children is derived from aspartame (Butchko and
Intake of phenylalanine from the normal diet compared to
Kotsonis, 1989, 1991, 1996) (Figs. 2 and 3). The only
that from aspartame (90th percentile, 14-day average, “eaters” only)
individuals who must be concerned regarding aspar-
adults (FDA, 1996b). Thus, acceptable dietary expo-
et al., 1990; Davis et al., 1991; Muir et al., 1994; Werner
sure to methanol is approximately 25 times potential
et al., 1995), not the typical age group of aspartame con-
exposure to methanol following 90th percentile con-
sumers. In addition, it is widely thought that apparent
increases in brain tumor rates in the mid-1980s may not
Recently, Trocho et al. (1998) concluded from a study
reflect genuine increases in brain tumors but rather en-
in rats that aspartame may be hazardous because
hanced detection, largely resulting from the availabil-
formaldehyde adducts in tissue proteins and nucleic
ity of sophisticated noninvasive diagnostic technology,
acids from aspartame may accumulate. However, ac-
such as CT and MRI (Boyle et al., 1990; Greig et al.,
cording to Tephly (1999), the doses of aspartame used
1990; Marshall, 1990; Davis et al., 1991; La Vecchia
in the study do not even yield blood methanol concentra-
et al., 1992; Modan et al., 1992; Muir et al., 1994; Werner
tions outside control values. Further, the amount of as-
et al., 1995; Legler et al., 1999).
partame equal to that in about 75 servings (12 oz) of bev-
Epidemiologists have criticized Olney and co-
erage as a single bolus for an adult human results in no
workers’ attempted association between the introduc-
detectable increase in blood formate concentrations in
tion of aspartame and occurrence of brain tumors
humans, whereas increased urinary formate excretion
(Davies et al., 1996; Ross, 1998). For example, Ross
shows that the body is well able to handle even excessive
stated, “From an epidemiologic perspective, the con-
amounts of aspartame. In addition, there is no accu-
clusion of this report may well represent a classic ex-
mulation of blood or urinary methanol or formate with
ample of ‘ecologic fallacy’ . . . There is no information
long-term exposure to aspartame. Thus, Tephly (1999)
available regarding whether the individuals who devel-
concluded, “the normal flux of one-carbon moieties
oped brain tumors consumed aspartame. For example,
whether derived from pectin, aspartame, or fruit juices
one might also invoke (a) cellular phone, home com-
is a physiologic phenomenon and not a toxic event.”
puter, and VCR usage; (b) depletion of the ozone layer;or (c) increased use of stereo headphones as potentially
Brain tumors. Olney et al. (1996) claimed that the
causative agents . . . some or all of these possibilities
reported increased rate of brain tumors in the United
may or may not have any biological plausibility to the
States may be associated with the marketing of aspar-
tame. However, according to Levy and Hedeker (1996),
In addition, a case-control study, which specifically
the arguments of Olney et al. implicitly require two bio-
evaluated aspartame consumption and the risk of child-
logically indefensible assumptions: first, that a certain
hood brain tumors, was published by Gurney et al.
factor (aspartame) could cause an observed increase in
(1997). In this study, case patients were 19 years of age
the incidence of brain cancer in less than 4 years and
or older and were diagnosed with a primary brain tu-
second, that even more widespread exposure to this fac-
mor between 1984 and 1991. The results of the study
tor would cause no further increase in the incidence of
showed that children with brain tumors were no more
that cancer in subsequent years. The fact is that the
likely to have consumed aspartame than control chil-
trend of increased brain tumor rates started well be-
dren, nor was there any elevated risk from maternal
fore aspartame was marketed, and overall brain tumor
consumption of aspartame during pregnancy.
rates have actually been decreasing since about 1990
Olney’s involvement with this issue began before as-
(Levy and Hedeker, 1996; National Cancer Institute,
partame approval in the United States when he claimed
to the FDA and the Public Board of Inquiry (PBOI), ap-
Further, the pattern of increased brain tumor rates
pointed by FDA to review his concerns (FDA, 1981),
has been noted primarily in the very elderly (Greig
that the results of studies in rats indicated that aspar-tame may cause brain tumors. At that time, he claimedthat aspartame-fed rats had a higher rate of brain tu-mors than control rats in one study and that anotherlifetime rat study, including in utero exposure to as-partame, was unreliable because the brain tumor inci-dence was too high in the control group. The underly-ing basis for such claims is the incorrect assertion thatthe background incidence of brain tumors in Sprague–Dawley (SD) rats is 0.1%; the actual background inci-dence is at least 20–30 times higher (Koestner, 1984,1997).
FDA (1981) concluded that there was no dose-
dependent increase in brain tumors or any expectedcharacteristic of carcinogens in the rat carcinogenic-
Yearly age-adjusted brain tumor rates from the National
ity studies. An additional study done in mice further
Cancer Institute SEER registry (1973–1996).
demonstrated that aspartame was not carcinogenic
SCIENTIFIC EVALUATION OF ASPARTAME IN THE POSTMARKETING PERIOD
(FDA, 1981), and a subsequent third, 2-year rat study
also confirmed that aspartame was not carcinogenic
Allegations regarding aspartame and adverse health
(Ishii, 1981, 1984). Thus, the results of three rat and
effects in the postmarketing period were evaluated
one mouse studies evaluating the carcinogenicity of as-
through additional scientific studies in both laboratory
partame demonstrate that aspartame is not a carcino-
animals and humans. The results of these studies con-
gen, even at dosages hundreds of times higher than
firmed the results of the previous studies demonstrat-
the 90th percentile of human consumption (FDA, 1981;
ing that aspartame is safe and not associated with ad-
Ishii, 1981, 1984; Cornell et al., 1984; Koestner, 1984,
Although the PBOI appointed by FDA to review
Olney’s concerns of neurotoxicity and brain tumors ini-
CONCLUSIONS
tially could not reach a decision regarding aspartameand brain tumors (FDA, 1980), the additional consid-
In accordance with regulatory requirements, prior to
erations and findings in animals summarized above
marketing, aspartame was demonstrated to be a safe
prompted a letter (Nauta, 1981) dated August 6, 1981,
sweetener for its intended uses based on the results of
to FDA Commissioner Hayes from Dr. Nauta, Chair-
over 100 scientific studies in animals and humans. In
man of the PBOI, who stated in regard to aspartame’s
the postmarketing period, the safety of aspartame was
approval by FDA: “. . . had we known earlier about
further confirmed through extensive monitoring of in-
the reassuring outcome of the recent Japanese onco-
take vs the ADI, postmarketing surveillance of anecdo-
genicity studies, our recommendation would doubtless
tal reports of adverse health effects, and postmarketing
have been for unqualified approval . . . we wish to ex-
research to evaluate these allegations and other scien-
press our endorsement of your final decision in this
tific issues in controlled, scientific studies.
The results of the intake studies, despite differences
The allegations by Olney and co-workers regarding
in methodology, demonstrated consistent intakes in var-
aspartame and brain tumors have been evaluated by
ious countries that were well below the ADI; anal-
scientists at government and regulatory agencies in
ysis of the postmarketing surveillance of consumer
the United States, the United Kingdom, the European
reports of adverse health effects revealed no consis-
tent pattern of symptoms that could be causally re-lated to consumption of aspartame; and the results of
—The U.S. National Cancer Institute (NCI) (1997)
scientific studies to evaluate these allegations did not
concluded, “a recent analysis of the NCI statistics on
show a causal relationship between aspartame and al-
cancer incidence in the United States does not support
leged adverse effects. Thus, the totality of scientific evi-
an association between the use of aspartame and an
dence clearly demonstrates that, even in amounts many
times what people typically consume, aspartame is safe
—The U.S. FDA concluded that the analysis “does not
(Stegink and Filer, 1984; American Medical Associa-
support an association between the use of aspartame
tion, 1985; Stegink, 1987a,b; Janssen and van der
and increased incidence of brain tumors” (FDA, 1996a).
Heijden, 1988; Butchko and Kotsonis, 1989; Fisher,
—In the UK, the Committee on Carcinogenicity at
1989; Sze, 1989; Fernstrom, 1991; Jobe and Dailey,
the Department of Health stated, “The Committee con-
1993; Lajtha et al., 1994; Tschanz et al., 1996).
cluded that the data published by Olney et al. did notraise any concerns with regard to the use of aspartamein the United Kingdom” (Department of Health, 1998;
REFERENCES
—The Scientific Committee for Food (1997) of the Eu-
Abrams, I. J. (1986). Using the menu census survey to estimate di-
ropean Union concluded, “. . . the data do not support
etary intake: Postmarket surveillance of aspartame. In Interna-
the proposed biphasic increase in the incidence of brain
tional Aspartame Workshop Proceedings, November 17–21, 1986,Marbella, Spain. International Life Sciences Institute—Nutrition
tumors in the USA during the 1980’s.”
Abrams, I. J. (1992). Using the menu census survey to estimate di-
(ANZFA, 1997) concluded, “From the extensive sci-
etary intake: postmarket surveillance of aspartame. In Food Safety
entific data available at this stage, the evidence does
Assessment (J. W. Finley, S. F. Robinson, and D. J. Armstrong, Eds.),
not support that aspartame is carcinogenic in either
pp. 201–213. Am. Chem. Soc., Washington, DC.
animals or humans. There appears to be no foundation
Agencia Saude. (1999). Forum of Scientific Discussion: Aspartame.
to recent USA reports of increased brain tumors in
Agencia Nacional de Vigilancia Sanitaria, Diretoria de Alimentose Toxicologia, Sao Paulo, Brazil. October 29, 1999.
American Medical Association (1985). Aspartame: A review of safety
—Finally, after an expert analysis, the Brazilian Min-
issues. JAMA 254, 400–402.
istry of Health concluded that aspartame does not cause
Amery, W. K. (1988). More on aspartame and headache. Headache 28,
ANZFA (1997). Aspartame: Information for Consumers, ANZFA
Cornell, R. G., Wolfe, R. A., and Sanders, P. G. (1984). Aspartame and
Information Paper 8. Australia New Zealand Food Authority,
brain tumors: Statistical issues. In Aspartame: Physiology and Bio-
Canberra, Australia, and Wellington, New Zealand. chemistry (L. D. Stegink and L. J. Filer, Eds.), pp. 459–479. Marcel
Aspinall, R. L., Saunders, R. N., Pautsch, W. F., and Nutting,
E. F. (1980). The biological properties of aspartame. V. Ef-
Dailey, J. W., Lasley, S. M., Mishra, P. K., Bettendorf, A. F.,
fects on a variety of physiological parameters related to in-
Burger, R. L., and Jobe, P. C. (1989). Aspartame fails to facilitate
flammation and metabolism. J. Environ. Pathol. Toxicol. 3,
pentylenetetrazol-induced convulsions in CD-1 mice. Toxicol. Appl.Pharmacol. 98, 475–486.
Bar, A., and Biermann, C. (1992). Intake of intense sweeteners in
Dailey, J. W., Lasley, S. S., Burger, R. L., Bettendorf, A. F., Mishra,
Germany. Z. Ernahrungswiss. 31, 25–39.
P. K., and Jobe, P. C. (1991). Amino-acids, monoamines and
Bergsten, C. (1993). Intake of Acesulfame-K, Aspartame, Cyclamate
audiogenic-seizures in genetically epilepsy-prone rats: Effects of
and Saccharin in Norway, SNT Report 3. Norwegian Food Control
aspartame. Epilepsy Res. 8, 122–133.
Davies, S. M., Ross, J. A., and Woods, W. G. (1996). Aspartame
Bianchi, R. G., Muir, E. T., Cook, D. L., and Nutting, E. F. (1980).
and brain tumors: Junk food science. In Causes Childhood Can-
The biological properties of aspartame. II. Actions involving the
cer Newsletter, Vol. 7. University of Minnesota, St. Paul, MN.
gastrointestinal system. J. Environ. Pathol. Toxicol. 3, 355–362.
Davis, D. L., Ahlbom, A., Hoel, D., and Percy, P. (1991). Is brain cancer
Boyle, P., Maisonneuve, P., Saracci, R., and Muir, C. S. (1990). Is the
mortality increasing in industrial countries? Am. J. Ind. Med. 19,
increased incidence of primary brain tumors in the elderly real?
J. Natl. Cancer Inst. 82, 1594–1596.
Department of Health, UK (1998). 1996 Annual Report of the Com-
Bradstock, M. K., Serdula, M. K., Marks, J. S., Barnard, R. J., Crane,
mittees on Toxicity, Mutagenicity, and Carcinogenicity of Chemicals
N. T., Remington, P. L., and Trowbridge, F. L. (1986). Evaluation of
in Food, Consumer Products and the Environment. The Stationery
reactions to food additives: The aspartame experience. Am. J. Clin.Nutr. 43, 464–469.
Diomede, L., Romano, M., Guiso, G., Caccia, S., Nava, S., and
Burns, T. S., Stargel, W. W., Tschanz, C., Kotsonis, F. N., and Hurwitz,
Salmona, M. (1991). Interspecies and interstrain studies on the in-
A. (1991). Aspartame and sucrose produce a similar increase in the
creased susceptibility to metrazol-induced convulsions in animals
plasma phenylalanine to large neutral amino-acid ratio in healthy-
given aspartame. Food Chem. Toxicol. 29, 101–106.
subjects. Pharmacology 43, 210–219.
Dodge, R. E., Warner, D., Sangal S, and O’Donnell RD (1990). The
Butchko, H. H., and Kotsonis, F. N. (1989). Aspartame: Review of
effect of single and multiple doses of aspartame on higher cognitive
recent research. Comments Toxicol. 3, 253–278.
performance in humans. Aviat. Space Environ. Med. May, A30.
Butchko, H. H., and Kotsonis, F. N. (1991). Acceptable daily intake
Faich, G. A. (1986). Adverse-drug-reaction monitoring. N. Engl. J.
vs actual intake: The aspartame example. J. Am. Coll. Nutr. 10, Med. 314, 1589–1592.
FDA (1974). Food additives permitted in food for human consumption.
Butchko, H. H. (1994). Adverse reactions to aspartame: Double-blind
Fed. Regist. 39, 27317–27320. [July 26, 1974]
challenge in patients from a vulnerable population” by Walton et al.
FDA (1980). Decision of the Public Board of Inquiry, Aspartame.Biol. Psychiatry 36, 206–207.
Butchko, H. H., and Kotsonis, F. N. (1994). Postmarketing surveil-
FDA (1981). Aspartame: Commissioner’s final decision. Fed. Regist.
lance in the food industry: The aspartame case study. In Nutri-46, 38285–38308. [July 24, 1981] tional Toxicology (F. N. Kotsonis, M. Mackey, and J. Hjelle, Eds.),
FDA (1984). Food additives permitted for direct addition to food
pp. 235–250. Raven Press, New York.
for human consumption: Aspartame. Fed. Regist. 49, 6672–6682.
Butchko, H. H., Tschanz, C., and Kotsonis, F. N. (1994). Postmarket-
ing surveillance of food additives. Regul. Toxicol. Pharmacol. 20,
FDA (1986). Food additives permitted for human consumption:
Aspartame. Fed. Regist. 51, 42999–43000. [November 28, 1986]
Butchko, H. H., and Kotsonis, F. N. (1996). Acceptable daily in-
FDA (1995). Summary of Adverse Reactions Attributed to Aspartame.
take and estimation of consumption. In The Clinical Evaluation
United States Food and Drug Administration, Washington, DC. of A Food Additive: Assessment of Aspartame (C. Tschanz, H. H. Butchko, W. W. Stargel, and F. N. Kotsonis, Eds.), pp. 43–53. CRC
FDA (1996a). FDA Statement on Aspartame, FDA Talk Paper T96–75,
November 18, 1996. United States Food and Drug Administration,Washington, DC.
Butchko, H. H., Tschanz, C., and Kotsonis, F. N. (1996). Postmar-
keting surveillance of anecdotal medical complaints. In The Clin-
FDA (1996b). Food additives permitted for direct addition to food
ical Evaluation of A Food Additive: Assessment of Aspartame
for human consumption: Dimethyl dicarbonate. Fed. Regist. 61,
(C. Tschanz, H. H. Butchko, W. W. Stargel, and F. N. Kotsonis, Eds.),
pp. 183–193. CRC Press, Boca Raton, FL.
Ferguson, H. B., Stoddart, C., and Simeon, J. G. (1986). Double-blind
Cain, D. P., Boon, F., and Bevan, M. (1989). Failure of aspartame
challenge studies of behavioral and cognitive effects of sucrose-
to affect seizure susceptibility in kindled rats. Neuropharmacology
aspartame ingestion in normal children. Nutr. Rev. 44, 144–150. 28, 433–435.
Fernstrom, J. D. (1991). Central nervous system effects of aspartame.
Camfield, P. R., Camfield, C. S., Dooley, J., Gordon, K., Jollymore, S.,
In Sugars and Sweeteners (N. Kretchmer and C. B. Hollenbeck,
and Weaver, D. F. (1992). Aspartame exacerbates EEG spike-wave
Eds.), pp. 151–173. CRC Press, Boca Raton, FL.
discharge in children with generalized absence epilepsy: A double-
Filer, L. J., Baker, G. L., and Stegink, L. D. (1983). Effect of aspartame
blind controlled study. Neurology 42, 1000–1003.
loading on plasma and erythrocyte free amino acid concentrations
Centers for Disease Control (1984). Evaluation of consumer com-
in one-year-old infants. J. Nutr. 113, 1591–1599.
plaints related to aspartame use. MMWR 33, 605–607.
Filer, L. J., and Stegink, L. D. (1989). Aspartame metabolism in nor-
Chambolle, M., Collerie de Borely, A., Renault, C., and Volatier,
mal adults, phenylketonuric heterozygotes, and diabetic subjects.
J. (1994). Intake of Intense Sweeteners in France (1989–Diabetes Care 12, 67–74. 1992). CREDOC, Departement Prospective de la Consommation,
Fisher, R. S. (1989). Aspartame, neurotoxicity, and seizures: A review. J. Epilepsy 2, 55–64.
SCIENTIFIC EVALUATION OF ASPARTAME IN THE POSTMARKETING PERIOD
Flamm, W. G. (1997). Increasing brain tumor rats: Is there a link to
Hoffman, R. (1973). Long Term Tolerance of Aspartame by Obese
aspartame? J. Neuropathol. Exp. Neurol. 56, 105–106. Adults, research report. G. D. Searle & Co., Skokie, IL. [Submit-
Frey, G. H. (1973). Long Term Tolerance of Aspartame by NormalAdults, research report. G. D. Searle & Co., Skokie, IL. [Submitted
Hulshof, K. F. A. M., and Bouman, M. (1995). Use of Various Types ofSweeteners in Different Population Groups:. 1992 Dutch National
Frey, G. H. (1976). Use of aspartame by apparently healthy children
Food Consumption Survey. TNO Nutrition and Food Research In-
and adolescents. J. Toxicol. Environ. Health 2, 401–415.
Garattini, S., Caccia, S., Romano, M., Diomed, L., Guiso, G.,
Ishii, H. (1981). Incidence of brain tumors in rats fed aspartame.
Vezzani, A., and Salmona, M. (1988). Studies on the suscep-
Toxicol. Lett. 7, 433–437.
tibility to convulsions in animals receiving abuse doses of as-
Ishii, H. (1984). Chronic feeding studies with aspartame and its dike-
partame. In Dietary Phenylalanine and Brain Function (R. J.
topiperazine. In Aspartame: Physiology and Biochemistry (L. D.
Wurtman and E. Ritter-Walker, Eds.), pp. 131–143. Birkhauser,
Stegink and L. J. Filer, Eds.), pp. 307–319. Dekker, New York.
Janssen, P. J. C. M., and van der Heijden, C. A. (1988). Aspartame:
Garnier-Sagne, I., Leblanc, J. C., and Verger, Ph. (2001). Calculation of
Review of recent experimental and observational data. Toxicology
the intake of three intense sweeteners in young insulin-dependent
50, 1–26.
diabetics. Food Chem. Toxicol. 39, 745–749.
JECFA (1980). Aspartame; Evaluation of Certain Food Additives,
Garriga, M. M., Berkebile, C., and Metcalfe, D. (1991). A combined
Technical Report Series 653, pp. 20–21. Joint FAO/WHO Ex-
single-blind, double-blind, placebo-controlled study to determine
pert Committee on Food Additives, World Health Organization,
the reproducibility of hypersensitivity reactions to aspartame. J. Allergy Clin. Immunol. 87, 821–827.
Jobe, P. C., Lasley, S. M., Burger, R. L., Bettendorf, A. F., Mishra,
Geha, R., Buckley, C. E., Greenberger, P., Patterson, R., Polmar, S.,
P. K., and Dailey, J. W. (1992). Absence of an effect of aspartame
Saxon, A., Rohr, A., Yang, W., and Drouin, M. (1993). Aspartame is
on seizures induced by electroshock in epileptic and non-epileptic
no more likely than placebo to cause urticaria/angioedema: Results
rats. Amino Acids 3, 155–172.
of a multicenter, randomized, double-blind, placebo-controlled,
Jobe, P., and Dailey, J. (1993). Aspartame and seizures. Amino Acids
crossover study. J. Allergy Clin. Immunol. 92, 513–520. 4, 197–235.
Goldman, J. A., Lerman, R. H., Contois, J. H., and Udall, J. N. (1986).
Knopp, R. H., Brandt, K., and Arky, R. A. (1976). Effects of aspar-
Behavioral effects of sucrose on preschool children. J. Abnorm.
tame in young persons during weight reduction. J. Toxicol. Environ.Child Psychol. 14, 565–577. Health 2, 417–428.
Greig, N. H., Ries, L. G., Yancik, R., and Rapoport, S. I. (1990). In-
Koch, R., Shaw, K. N. F., Williamson, M., and Haber, M. (1976). Use
creasing annual incidence of primary malignant brain tumors in
of aspartame in phenylketonuric heterozygous adults. J. Toxicol.
the elderly. J. Natl. Cancer Inst. 82, 1621–1624. Environ. Health 2, 453–457.
Guiso, G., Caccia, S., Vezzani, A., Stasi, M. A., Salmona, M., Romano,
Koehler, S. M., and Glaros, A. (1988). The effect of aspartame on mi-
M., and Garattini, S. (1988). Effect of aspartame on seizures in
graine headache. Headache 28, 10–14.
various models of experimental epilepsy. Toxicol. Appl. Pharmacol.
Koestner, A. (1984). Aspartame and brain tumors: Pathology issues. 96, 485–493.
In Aspartame: Physiology and Biochemistry (L. D. Stegink and
Guiso, G., Diomede, M., Romano, S., Caccia, S., Sarati, A., and
L. J. Filer, Eds.), pp. 447–457. Dekker, New York.
Salmona, M. (1991). Effect of tyrosine on the potentiation by aspar-
Koestner, A. (1997). Increasing brain tumor rate: Is there a link to
tame and phenylalanine of metrazol-induced convulsions in rats.
aspartame? J. Neuropathol. Exp. Neurol. 56, 107–109. Food Chem. Toxicol. 29, 855–857.
Kotsonis, F. N., and Hjelle, J. J. (1996). The safety assessment of
Gurney, J. G., Pogoda, J. M., Holly, E. A., Hecht, S. S., and Preston-
aspartame: Scientific and regulatory considerations. In The Clin-
Martin, S. (1997). Aspartame consumption in relation to childhood
ical Evaluation of A Food Additive: Assessment of Aspartame
brain tumor risk: Results from a case-control study. J. Natl. Cancer
(C. Tschanz, H. H. Butchko, W. W. Stargel, and F. N. Kotsonis, Eds.),
Inst. 89, 1072–1074.
Health and Welfare Canada (1979). Proposal on Aspartame, Informa-
Kruesi, M. J. P., Rapoport, J. L., Cummings, E. M., Berg, C. J., Ismond,
tion Letter No. 564. Health Protection Branch, Health and Welfare
D. R., Flament, M., Yarrow, M., and Zahn-Waxler, C. (1987). Effects
of sugar and aspartame on aggression and activity in children. Am.
Helali, N. Y., El-Kashef, H., Salem, H., Gamiel, N., and Elmazar, M. M. J. Psychiatry 144, 1487–1490.
A. (1996). The effect of aspartame on seizure susceptibility and the
Kulczycki, A. (1986). Aspartame-induced urticaria. Ann. Intern. Med.
anticonvulsant action of ethosuximide, valproate and phenytoin in
104, 207–208.
mice. Saudi Pharm. J. 4, 149–156.
La Vecchia, C., Lucchini, F., Negri, E., Boyle, P., Maisonneuve, P., and
Heybach, J. P., and Smith, J. L. (1988). Intake of aspartame in 19–
Levi, F. (1992). Trends of cancer mortality in Europe, 1955–1989.
50 year old women from the USDA continuing survey of food intakes
IV, urinary tract, eye, brain and nerves, and thyroid. Eur. J. Cancer
by individuals (CSFII 85). FASEB J. 2, A1615. 28A, 1210–1281.
Heybach, J. P., and Allen, S. S. (1988). Resources for inferential esti-
Lajtha, A., Reilly, M. A., and Dunlop, D. S. (1994). Aspartame con-
mates of aspartame intake in the United States. In Dietary Pheny-
sumption: lack of effects on neural function. J. Nutr. Biochem. 5, lalanine and Brain Function (R. J. Wurtman and E. Ritter-Walker,
Eds.), pp. 365–372. Birkhauser, Boston.
Langlois, K. (1972). Short Term Tolerance of Aspartame by Normal
Heybach, J., and Ross, C. (1989). Aspartame consumption in a repre-
Adults, research report. G. D. Searle & Co., Skokie, IL. [Submitted
sentative sample of Canadians. J. Can. Diet. Assoc. 50, 166–170.
Hinson, A. L., and Nicol, W. M. (1992). Monitoring sweetener con-
Lapierre, K. A., Greenblatt, D. J., Goddard, J. E., Harmatz, J. S., and
sumption in Great Britain. Food Addit. Contam. 9, 669–680.
Shader, R. I. (1990). The neuropsychiatric effects of aspartame in
Hoffman, R. (1972). Short Term Tolerance of Aspartame by Obese
normal volunteers. J. Clin. Pharmacol. 30, 454–460. Adults, research report. G. D. Searle & Co., Skokie, IL. [Submit-
Leclercq, C., Berardi, D., Sorbillo, M. R., and Lambe, J. (1999). Intake
of saccharin, aspartame, acesulfame K and cyclamate in Italian
teenagers: Present levels and projections. Food Addit. Contam. 16,
Olney, J. W., Farber, N. B., Spitznagel, E., and Robins, L. N. (1996).
Increasing brain tumor rates: Is there a link to aspartame? J. Neu-
Legler, J. M., Gloeckler Ries, L. A., Smith, M. A., Warren, J. L.,
ropathol. Exp. Neurol. 55, 1115–1123.
Heineman, E. F., Kaplan, R. S., and Linet, M. S. (1999). Brain and
Perego, C., DeSimoni, M. G., Fodritto, F., Raimondi, L., Diomede, L.,
other central nervous system cancers: Recent trends in incidence
Salmona, M., Algeri, S., and Garattini, S. (1988). Aspartame and
and mortality. J. Natl. Cancer Inst. 91, 1382–1390.
the rat brain monoaminergic system. Toxicol. Lett. 44, 331–339.
Lennon, H. D., Metcalf, L. E., Mares, S. E., Smith, J. H., Nutting,
Pinto, J. M. B., and Maher, T. J. (1988). Administration of aspartame
E. F., and Saunders, F. J. (1980). The biological properties of aspar-
potentiates pentylenetetrazole- and fluorothyl-induced seizures in
tame. IV. Effects on reproduction and lactation. J. Environ. Pathol.
mice. Neuropharmacology 27, 51–55. Toxicol. 3, 375–386.
Potts, W. J., Bloss, J. L., and Nutting, E. F. (1980). The biological
Leon, A. S., Hunninghake, D. B., Bell, C., Rassin, D. K., and Tephly,
properties of aspartame. I. Evaluation of central nervous system
T. R. (1989). Safety of long-term large doses of aspartame. Arch.
effects. J. Environ. Pathol. Toxicol. 3, 341–353. Intern. Med. 149, 2318–2324.
Raines, A. (1987). Another side to aspartame Wash. Post Health
Levy, P. S., Hedeker, D., and Sanders, P. G. (1995). Aspartame and
June 2. [Letter]
headache. Neurology 45, 1631–1632.
Ranney, R. E., Oppermann, J. A., Muldoon, E., and McMahon, F. G.
Levy, P. S., and Hedeker, D. (1996). Statistical and epidemiological
(1976). Comparative metabolism of aspartame in experimental an-
treatment of the SEER incidence data. J. Neuropathol. Exp. Neurol.
imals and humans. J. Toxicol. Environ. Health 2, 441–451. 55, 1280.
Reilly, M. A., Debler, E. A., Fleischer, A., and Lajtha, A. (1989). Lack
Lieberman, H. R., Caballero, B., Emde, G. G., and Bernstein, J. G.
of effect of chronic aspartame ingestion on aminergic receptors in
(1988). The effects of aspartame on human mood, performance,
rat brain. Biochem. Pharmacol. 38, 4339–4341.
and plasma amino acid levels. In Dietary Phenylalanine and Brain
Reilly, M. A., Debler, E. A., and Lajtha, A. (1990). Perinatal exposure
Function (R. J. Wurtman and E. Ritter-Walker, Eds.), pp.196–200.
to aspartame does not alter aminergic neurotransmitter systems in
weanling rat brain. Res. Commun. Psychol. Psychiatry Behav. 15,
Lu, F. C. (1988). Acceptable daily intake: Inception, evolution, and
application. Regul. Toxicol. Pharmacol. 8, 45–60.
Renwick, A. G. (1990). Acceptable daily intake and the regulation of
MAFF. (1990). Intakes of intense and bulk sweeteners in the UK
intense sweeteners. Food Addit. Contam. 7, 463–475.
1987–1988. Food Surveillance Paper No. 29. Ministry of Agricul-
Renwick, A. G. (1991). Safety factors and establishment of acceptable
ture, Fisheries and Food, London, UK.
daily intakes. Food Addit Contam. 8, 135–149.
MAFF (1995). Survey of the Intake of Sweeteners by Diabetics, Food
Ross, J. A. (1998). Brain tumors and artificial sweeteners? A lesson
Surveillance Info. Sheet. Ministry of Agriculture, Fisheries and
on not getting soured on epidemiology. Med. Pediatr. Oncol. 30, 7–8.
Food, Food Safety Directorate. London, UK.
Rowan, A. J., Shaywitz, B. A., Tuchman, L., French, J. A., Luciano,
MAFF (1999). Aspartame. Ministry of Agriculture, Fisheries
D., and Sullivan, C. M. (1995). Aspartame and seizure susceptibil-
and Food, Department of Health and the Scottish Executive.
ity: Results of a clinical study in reportedly sensitive individuals.
[http://www.foodstandards.gov.uk/maff/archive/food/asp9911.htm]
Epilepsia 36, 270–275.
Marshall, E. (1990). Experts clash over cancer data. Science 250,
Ryan-Harshman, M., Leiter, L. A., and Anderson, G. H. (1987). Pheny-
lalanine and aspartame fail to alter feeding behavior, mood and
Martin-Du Pan, R., Mauron, C., Glaeser, B., and Wurtman, R. J.
arousal in men. Physiol. Behav. 39, 247–253.
(1982). Effect of various oral glucose doses on plasma neutral amino
Saravis, S., Shachar, R., Zlotkin, S., Leiter, L. A., and Anderson,
acid levels. Metabolism 31, 937–943.
G. H. (1990). Aspartame: Effects on learning, behavior, and mood.
Meldrum, B. S., Nanji, N., and Cornell, R. G. (1989). Lack of effect of
Pediatrics 86, 75–83.
aspartame or of l-phenylalanine on photically induced myoclonus
Saunders, F. J., Pautsch, W. F., and Nutting, E. F. (1980). The biolog-
in the baboon, Papio papio. Epilepsy Res. 4, 1–7.
ical properties of aspartame. III. Examination for endocrine-like
Milich, R., and Pelham, W. E. (1986). Effects of sugar ingestion on the
activities. J. Environ. Pathol. Toxicol. 3, 363–373.
classroom and playgroup behavior of attention deficit disordered
Schiffman, S. S., Buckley, C. E., Sampson, H. A., Massey, E. W.,
boys. J. Consult. Clin. Psychol. 54, 714–718.
Baraniuk, J. N., Follett, J. V., and Warwick, Z. S. (1987). Aspar-
Modan, B., Wagener, D. K., Feidman, J. J., Rosenberg, H. M., and
tame and susceptibility to headache. N. Engl. J. Med. 317, 1181–
Fainleib, M. (1992). Increased mortality from brain tumors: A com-
bined outcome of diagnostic technology and change of attitude to-
Schiffman, S. S. (1988). Aspartame and headache. Headache 28, 370.
ward the elderly. Am. J. Epidemiol. 135, 1349–1357.
Schiffman, S. (1995). Aspartame and headache. Neurology 45, 1632.
Molinary, S. V. (1984). Preclinical studies of aspartame in nonprimate
Schomer, D. L., Spiers, P., and Sabounjian, L. A. (1996). Evaluation
animals. In Aspartame: Physiology and Biochemistry (L. D. Stegink
of behavior, cognition, mood, and electroencephalograms in normal
and L. J. Filer, Eds.), pp. 289–306. Marcel Dekker, New York.
adults and potentially vulnerable populations. In The Clinical Eval-
Muir, C. S., Storm, H. H., and Polednak, A. (1994). Brain and other
uation of a Food Additive: Assessment of Aspartame (C. Tschanz,
nervous system tumours. Cancer Surv. 19/20, 369–92.
H. H. Butchko, W. W. Stargel, and F. N. Kotsonis, Eds.), pp. 217–233.
National Cancer Institute (1997). Cancer Facts. Artificial Sweeteners,
April 9, 1997 (http://cis.nci.nih.gov/fact/3 19.htm).
Scientific Committee for Food (1985). Food-Science and Techniques:
National Cancer Institute (1999). Brain and other nervous system
Reports of the Scientific Committee for Food, sixteenth series. Com-
cancer (invasive). In SEER Cancer Statistics Review 1973–1996.
mission of the European Communities, Luxembourg.
Scientific Committee for Food (1997). Aspartame. In Extract of Min-
National Food Authority Australia (1995). Survey of Intense Sweet-utes of the 107th Meeting of the Scientific Committee for Food Heldener Consumption in Australia: Final Report. National Food Au-
on June 12–13, 1997, in Brussels, pp. 9–10. European Commission,
Nauta, W. J. H. (1981). Letter to FDA Commisioner Hayes, August 6,
Shaywitz, B. A., and Novotny, E. J. (1993). Aspartame and seizures. Neurology 43, 630.
SCIENTIFIC EVALUATION OF ASPARTAME IN THE POSTMARKETING PERIOD
Shaywitz, B. A., Sullivan, C. M., Anderson, G. M., Gillespie, S. M.,
Tephly, T. R. (1999). Comments on the purported generation of
Sullivan, B., and Shaywitz, S. E. (1994a). Aspartame, behavior, and
formaldehyde and adduct formation from the sweetener aspartame.
cognitive function in children with attention deficit disorder. Pedi-Life Sci. 65, 157–160. atrics 93, 70–75.
Tilson, H. A., Thai, L., Zhao, D., Sobotka, T. J., and Hong, J. S. (1989).
Shaywitz, B. A., Anderson, G. M., Novotny, E. J., Ebersole, J. S.,
Oral administration of aspartame is not proconvulsant in rats. Neu-
Sullivan, C. M., and Gillespie, S. M. (1994b). Aspartame has no
rotoxicology 10, 229–238.
effect on seizures or epileptiform discharges in epileptic children.
Toledo, M. C. F., and Ioshi, S. H. (1995). Potential intake of intense
Ann. Neurol. 35, 98–103.
sweeteners in Brazil. Food Addit. Contam. 12, 799–808.
Sperber, E. F., Moshe, S. L., and Dow-Edwards, D. L. (1995). Prena-
Tollefson, L. (1988). Monitoring adverse reactions to food additives in
tal exposure to aspartame and seizure susceptibility. J. Epilepsy 8,
the U.S. Food and Drug Administration. Regul. Toxicol. Pharmacol.8, 438–446.
Spiers, P. A., Sabaounjian, L., Reiner, A., Myers, D. K., Wurtman,
Tollefson, L., Barnard, R. J., and Glinsmann, W. H. (1988). Monitor-
J., and Schomer, D. L. (1998). Aspartame: Neuropsychologic and
ing of adverse reactions to aspartame reported to the U.S. Food
neurophysiologic evaluation of acute and chronic effects. Am. J.
and Drug Administration. In Dietary Phenylalanine and BrainClin. Nutr. 68, 531–537. Function. (R. J. Wurtman and E. Ritter-Walker, Eds.), pp. 317–337.
Stegink, L. D., Filer, L. J., Jr., and Baker, G. L. (1977). Effect of as-
partame and aspartate loading upon plasma and erythrocyte free
Tollefson, L., and Barnard, R. J. (1992). An analysis of FDA passive
amino acid levels in normal adult volunteers. J. Nutr. 107, 1837–
surveillance reports of seizures associated with consumption of as-
partame. J. Am. Diet. Assoc. 92, 598–601.
Stegink, L. D., Filer, L. J., Baker, G. L., and McDonnell, J. E. (1979a).
Trefz, F., de Sonneville, L., Matthis, P., Benninger, C., Lanz-Englert,
Effect of aspartame loading upon plasma and erythrocyte amino
B., and Bickel, H. (1994). Neuropsychological and biochemical in-
acid levels in phenylketonuric heterozygotes and normal adult sub-
vestigations in heterozygotes for phenylketonuria during ingestion
jects. J. Nutr. 109, 708–717.
of high dose aspartame (a sweetener containing phenylalanine).
Stegink, L. D., Filer, L. J., and Baker, G. L. (1979b). Plasma erythro-
Hum. Genet. 93, 369–374.
cyte and human milk levels of free amino acids in lactating women
Trocho, C., Pardo, R., Rafecas, I., Virgili, J., Remesar, X., Fernandez-
administered aspartame or lactose. J. Nutr. 109, 2173–2181.
Lopez, J. A., and Alemany, M. (1998). Formaldehyde derived from
Stegink, L. D., Filer, L. J., Baker, G. L., and McDonnell, J. E. (1980).
dietary aspartame binds to tissue components in vivo. Life Sci. 63,
Effect of an abuse dose of aspartame upon plasma and erythrocyte
levels of amino acids in phenylketonuric heterozygous and normal
Tschanz, C., Butchko, H. H., Stargel, W. W., and Kotsonis, F. N. (Eds.)
adults. J. Nutr. 110, 2216–2224.
(1996). The Clinical Evaluation of A Food Additive: Assessment of
Stegink, L. D., Brummel, M. C., McMartin, K., Martin-Amat, G., Filer,
Aspartame. CRC Press, Boca Raton, FL.
L. J., Baker, G. L., and Tephly, T. R. (1981a). Blood methanol con-
Van Den Eeden, S. K., Koepsell, T. D., Longstreth, W. T., van Bell,
centrations in normal adult subjects administered abuse doses of
G., Daling, J. R., and McKnight, B. (1994). Aspartame ingestion
aspartame. J. Toxicol. Environ. Health 7, 281–290.
and headaches: A randomized crossover trial. Neurology 44, 1787–
Stegink, L. D., Filer, L. J., and Baker, G. L. (1981b). Plasma and ery-
throcyte concentrations of free amino acids in adult humans ad-
Virtanen, S. M., Rasanen, L., Paganus, A., Varo, P., and Akerblom,
ministered abuse doses of aspartame. J. Toxicol. Environ. Health
H. K. (1988). Intake of sugars and artificial sweeteners by adoles-
7, 291–305.
cent diabetics. Nutr. Rep. Int. 38, 1211–1218.
Stegink, L. D., Brummel, M. C., Filer, L. J., and Baker, G. L. (1983).
Walton, R. G., Hudak, R., and Green-Waite, R. J. (1993). Adverse
Blood methanol concentrations in one-year-old infants adminis-
reactions to aspartame: Double-blind challenge in patients from a
tered graded doses of aspartame. J. Nutr. 113, 1600–1606.
vulnerable population. Biol. Psychiatry 34, 13–17.
Stegink, L. D., and Filer, L. J. (Eds.) (1984). Aspartame: Physiology
Werner, M. H., Phuphanich, S., and Lyman, G. H. (1995). The in-
and Biochemistry. Marcel Dekker, New York.
creasing incidence of malignant gliomas and primary central-
Stegink, L. D. (1987a). Aspartame: Review of the safety issues. Food
nervous-system lymphoma in the elderly. Cancer 76, 1634– Technol. 41, 119–121.
Stegink, L. D. (1987b). The aspartame story: A model for the clinical
Wolf-Novak, L. C., Stegink, L. D., Brummel, M. C., Persoon,
testing of a food additive. Am. J. Clin. Nutr. 46, 204–215.
T. J., Filer, L. J., Bell, E. F., Ziegler, E. E., and Krause,
Stegink, L. D., Wolf-Novak, L. C., Filer, L. J., Bell, E. F., Zeigler, E. E.,
W. L. (1990). Aspartame ingestion with and without carbohydrate
Krause, W. L., and Brummel, M. C. (1987). Aspartame-sweetened
in phenylketonuric and normal subjects: Effect on plasma concen-
beverage: Effect on plasma amino acid concentrations in normal
trations of amino acids, glucose, and insulin. Metabolism 39, 391–
adults and adults heterozygous for phenylketonuria. J. Nutr. 117,
Wolraich, M., Milich, R., Stumbo, P., and Schultz, F. (1985). Effects
Stern, S. B., Bleicher, S. J., Flores, A., Gombos, G., Recitas, D.,
of sucrose ingestion on the behavior of hyperactive boys. J. Pediatr.
and Shu, J. (1976). Administration of aspartame in non-insulin-
106, 675–682.
dependent diabetics. J. Toxicol. Environ. Health 2, 429–439.
Wolraich, M. L., Lindgren, S. D., Stumbo, P. J., Stegink, L. D.,
Stokes, A. F., Belger, A., Banich, M. T., and Taylor, H. (1991). Effects
Appelbaum, M. I., and Kiritsy, M. C. (1994). Effects of diets high in
of acute aspartame and acute alcohol ingestion upon the cognitive
sucrose or aspartame on the behavior and cognitive performance of
performance of pilots. Aviat. Space Environ. Med. 62, 648–653.
children. N. Engl. J. Med. 330, 301–307.
Stokes, A. F., Belger, A., Banich, M. T., and Bernadine, E. (1994). Ef-
Wurtman, R. J. (1983). Neurochemical changes following high-dose
fects of alcohol and chronic aspartame ingestion upon performance
aspartame with dietary carbohydrates. N. Engl. J. Med. 309, 429–
in aviation relevant cognitive tasks. Aviat. Space Environ. Med. 65,
Zhi, J., and Levy, G. (1989). Aspartame and phenylalanine do not
Sze, P. Y. (1989). Pharmacological effects of phenylalanine on seizure
enhance theophylline-induced seizure in rats. Res. Commun. Chem.
susceptibility. Neurochem. Res. 14, 103–111. Pathol. Pharmacol. 66, 171–174.
Entretien avec Claude Prey par Michel Rostain / Lyrica n°70, 1981 D'opéra de chambre en opéra épistolaire , L'Escalier de Chambord ne nous dit pas autreClaude Prey s'est imposé en France commechose quand il convoque cinq chanteurs lyriquesl'auteur lyrique contemporain le plus joué. Lepour chanter le rôle de cinq chanteurs réunis surGrand Théâtre de Tours va créer le
Poisons Act 1971 Section 27 Poisons Regulation 2002 62(2)(a) APPLICATION FOR A LICENCE TO SELL OR SUPPLY CERTAIN SUBSTANCES To the Minister for Health and Health Services I, . (name, address and nature of business) hereby apply for a licence/renewal of licence to sell or supply the following substances to which Section 27 of the Poisons Act 1971 applies: SCH
 Regulatory Toxicology and Pharmacology 34, 221–233 (2001)
Regulatory Toxicology and Pharmacology 34, 221–233 (2001)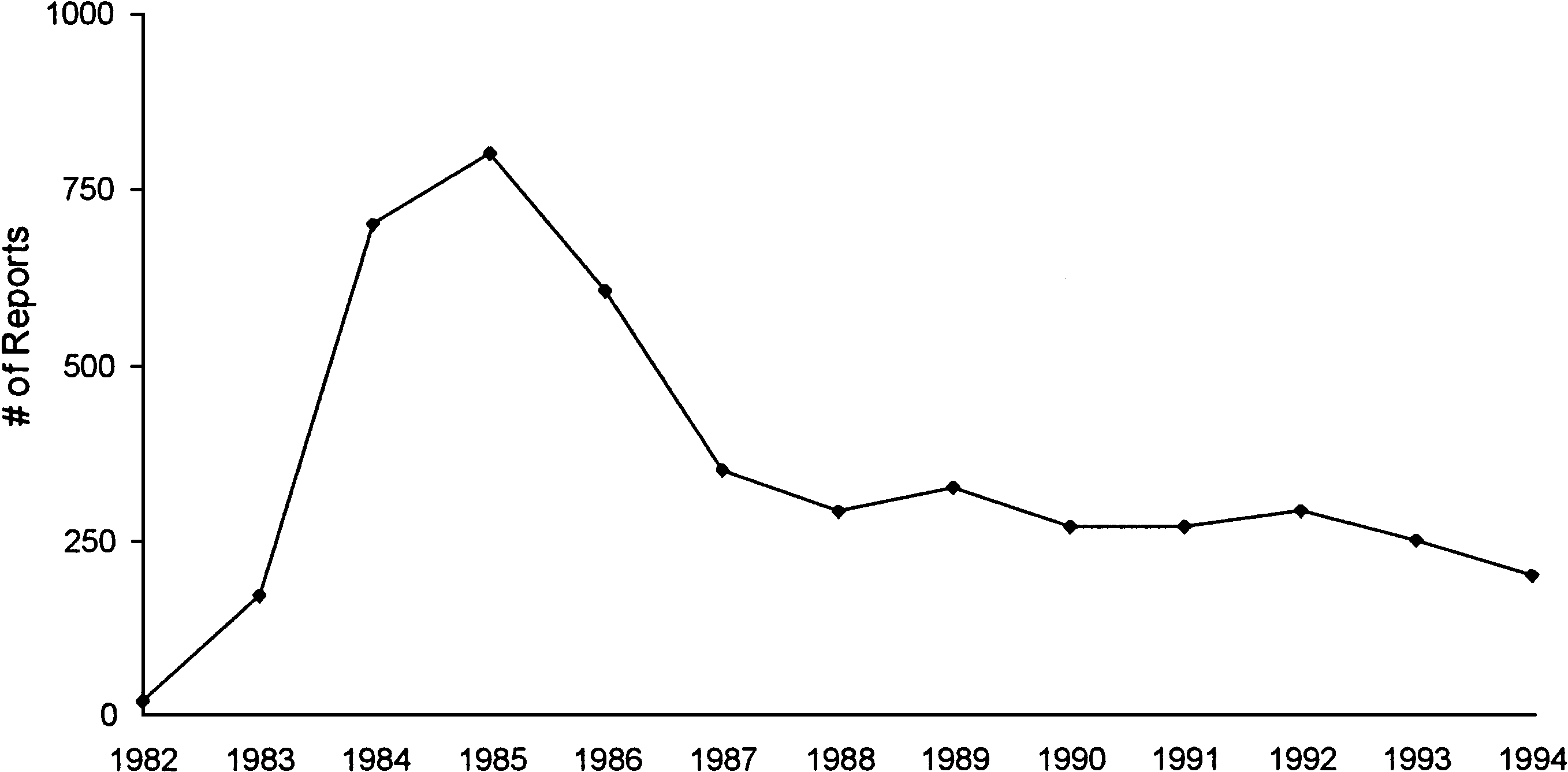 SCIENTIFIC EVALUATION OF ASPARTAME IN THE POSTMARKETING PERIOD
Headache topped the list of symptoms reported,
mid-1980s had a significant impact on the number of
followed by dizziness, mood changes, and nausea/
anecdotal reports. As seen in Fig. 1, the number of re-
vomiting. The report noted the decline, since the peak in
ports increased markedly during that time and, as the
1985, of reports from consumers regarding aspartame
controversy decreased in the late 1980s and early 1990s,
and further stated, “In summary, the number of adverse
reaction complaints received by the FDA and the nature
As there are more than 100 million aspartame users
of these reports in terms of demographic distribution,
in the United States, it is inevitable that some of them
severity, strength of association with the product, and
will experience medical ailments temporally associated
symptoms remain comparable to those from previous
with consumption of an aspartame-containing product
simply by chance. A temporal association does not mean
FDA also separately analyzed the 251 reports of
a causal association. The error of associating causal-
seizure anecdotally associated with aspartame con-
ity to coincidence is perhaps best stated by one scien-
sumption received through ARMS from 1986 to 1990
tist who stated, “As aspartame is estimated to be con-
and concluded that almost half were highly unlikely to
sumed by about half the U.S. population, one need not
be related to aspartame (Tollefson and Barnard, 1992).
SCIENTIFIC EVALUATION OF ASPARTAME IN THE POSTMARKETING PERIOD
Headache topped the list of symptoms reported,
mid-1980s had a significant impact on the number of
followed by dizziness, mood changes, and nausea/
anecdotal reports. As seen in Fig. 1, the number of re-
vomiting. The report noted the decline, since the peak in
ports increased markedly during that time and, as the
1985, of reports from consumers regarding aspartame
controversy decreased in the late 1980s and early 1990s,
and further stated, “In summary, the number of adverse
reaction complaints received by the FDA and the nature
As there are more than 100 million aspartame users
of these reports in terms of demographic distribution,
in the United States, it is inevitable that some of them
severity, strength of association with the product, and
will experience medical ailments temporally associated
symptoms remain comparable to those from previous
with consumption of an aspartame-containing product
simply by chance. A temporal association does not mean
FDA also separately analyzed the 251 reports of
a causal association. The error of associating causal-
seizure anecdotally associated with aspartame con-
ity to coincidence is perhaps best stated by one scien-
sumption received through ARMS from 1986 to 1990
tist who stated, “As aspartame is estimated to be con-
and concluded that almost half were highly unlikely to
sumed by about half the U.S. population, one need not
be related to aspartame (Tollefson and Barnard, 1992).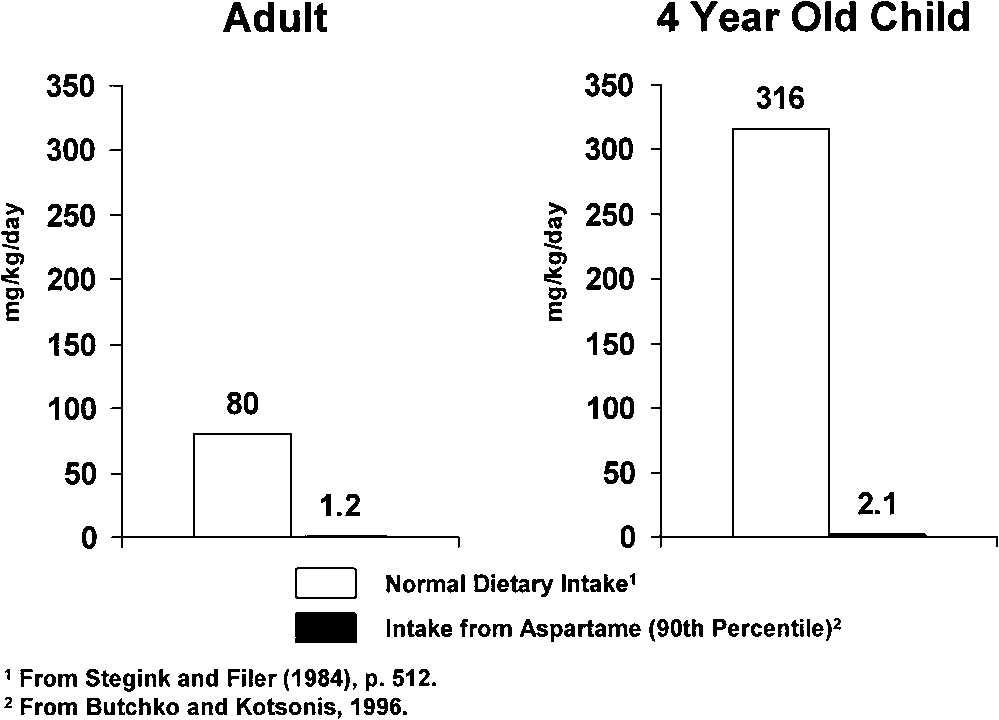
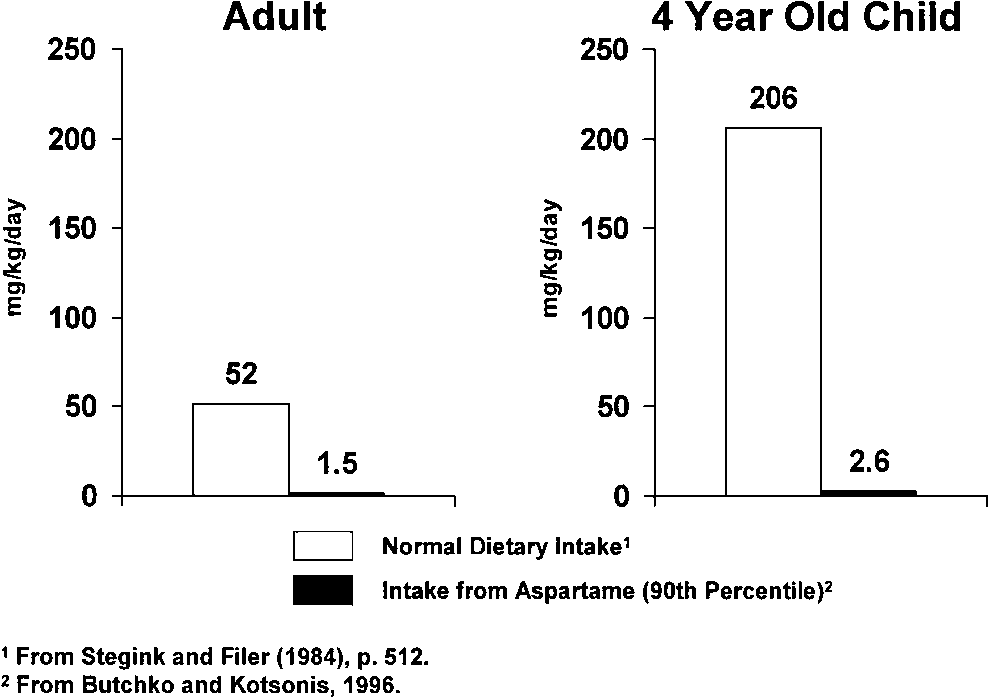 SCIENTIFIC EVALUATION OF ASPARTAME IN THE POSTMARKETING PERIOD
complaints to show a statistically significant result,as there were no differences between aspartame andplacebo in specific types of complaints.
SCIENTIFIC EVALUATION OF ASPARTAME IN THE POSTMARKETING PERIOD
complaints to show a statistically significant result,as there were no differences between aspartame andplacebo in specific types of complaints.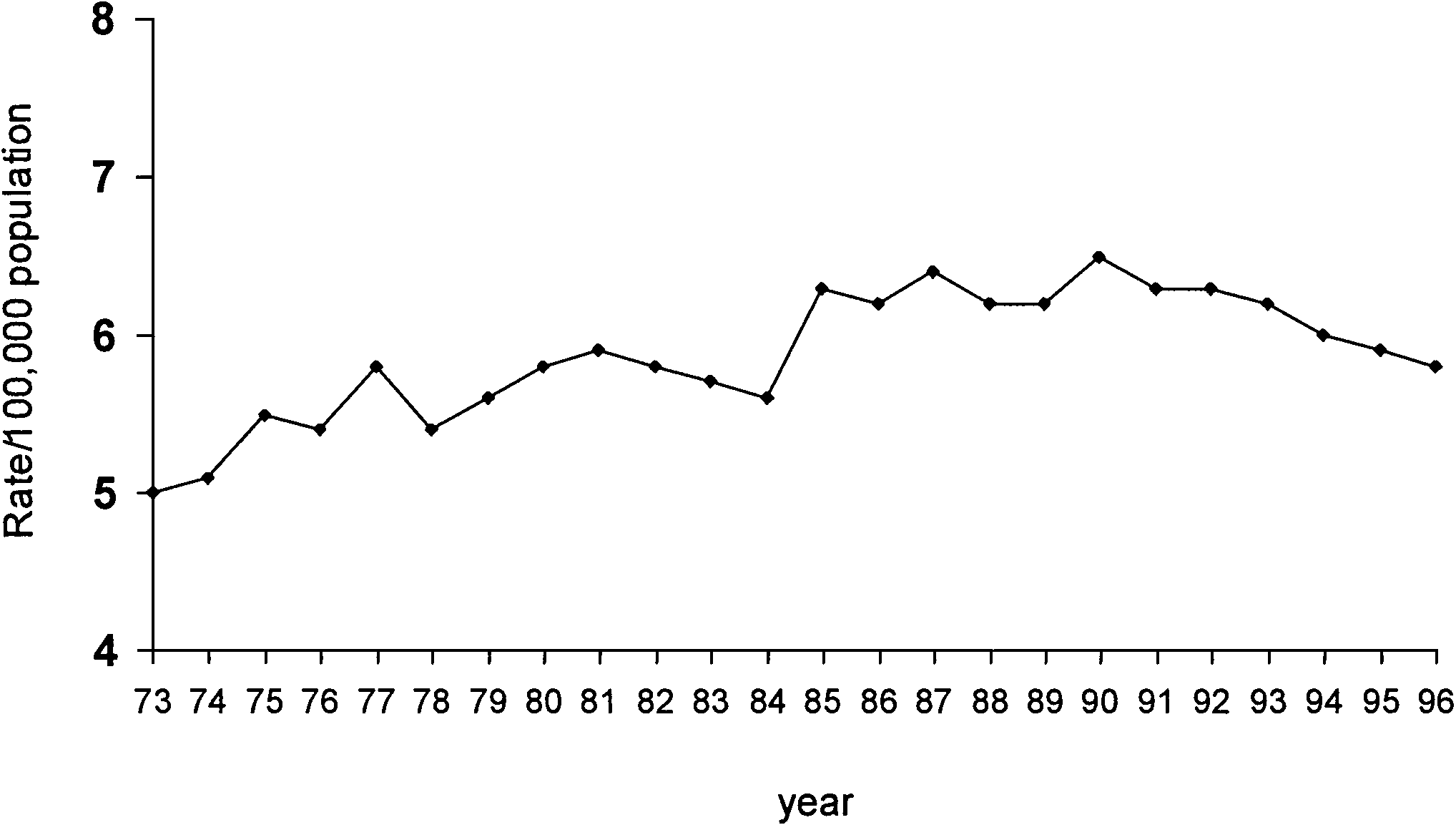 adults (FDA, 1996b). Thus, acceptable dietary expo-
et al., 1990; Davis et al., 1991; Muir et al., 1994; Werner
sure to methanol is approximately 25 times potential
et al., 1995), not the typical age group of aspartame con-
exposure to methanol following 90th percentile con-
sumers. In addition, it is widely thought that apparent
increases in brain tumor rates in the mid-1980s may not
Recently, Trocho et al. (1998) concluded from a study
reflect genuine increases in brain tumors but rather en-
in rats that aspartame may be hazardous because
hanced detection, largely resulting from the availabil-
formaldehyde adducts in tissue proteins and nucleic
ity of sophisticated noninvasive diagnostic technology,
acids from aspartame may accumulate. However, ac-
such as CT and MRI (Boyle et al., 1990; Greig et al.,
cording to Tephly (1999), the doses of aspartame used
1990; Marshall, 1990; Davis et al., 1991; La Vecchia
in the study do not even yield blood methanol concentra-
et al., 1992; Modan et al., 1992; Muir et al., 1994; Werner
tions outside control values. Further, the amount of as-
et al., 1995; Legler et al., 1999).
adults (FDA, 1996b). Thus, acceptable dietary expo-
et al., 1990; Davis et al., 1991; Muir et al., 1994; Werner
sure to methanol is approximately 25 times potential
et al., 1995), not the typical age group of aspartame con-
exposure to methanol following 90th percentile con-
sumers. In addition, it is widely thought that apparent
increases in brain tumor rates in the mid-1980s may not
Recently, Trocho et al. (1998) concluded from a study
reflect genuine increases in brain tumors but rather en-
in rats that aspartame may be hazardous because
hanced detection, largely resulting from the availabil-
formaldehyde adducts in tissue proteins and nucleic
ity of sophisticated noninvasive diagnostic technology,
acids from aspartame may accumulate. However, ac-
such as CT and MRI (Boyle et al., 1990; Greig et al.,
cording to Tephly (1999), the doses of aspartame used
1990; Marshall, 1990; Davis et al., 1991; La Vecchia
in the study do not even yield blood methanol concentra-
et al., 1992; Modan et al., 1992; Muir et al., 1994; Werner
tions outside control values. Further, the amount of as-
et al., 1995; Legler et al., 1999).