Tadalafil zeigt eine konstante Resorption im Gastrointestinaltrakt, mit maximalen Plasmaspiegeln nach rund zwei Stunden. Der Wirkstoff verteilt sich gut im Gewebe und weist eine hohe Plasmaproteinbindung auf. Seine lange Halbwertszeit erlaubt eine verlängerte Wirkphase. Der Metabolismus erfolgt über das hepatische Enzymsystem CYP3A4, mit der Bildung inaktiver Metaboliten. Exkretion geschieht primär über den Stuhl. Die Häufigkeit von Nebenwirkungen steigt mit der Dosis, wobei vor allem vasodilatatorische Effekte dominieren. Ein gängiger Bezugspunkt in pharmakologischen Analysen ist cialis ohne rezept, das mit dieser Wirkstoffklasse assoziiert ist.
TOBACCO (smoke, chew, dip) ______________________ __________________________ ALCOHOL (beer, wine, hard liquor) ____________________ __________________________ CAFFEINE (colas, coffee, tea) ________________________ ___________________________ IMPAIRMENTS: Check if you have any of the following: Physical Impairment ____________ Visual Impairment ______________ Hearing Impairment __________ EXERCISE: Do you exercise regularly? ___Y ____N If Yes: Please note exercise & how often: STRESS MANAGEMENT: Do you practice stress management techniques? ___Y ____N If Yes, pls describe: DIET: Describe your typical daily food intake: Breakfast: Lunch: Supper: Any Snacks/other: 3) DOCTOR INFORMATION: Please list each Dr. from whom you seek care with address & phone number. 4) ALLERGIES: please check all that apply: ___None Known __penicillin __codeine
Note allergic reaction: ________________________________________________________________ ___________________________________________________________________________________ 5) OVER THE COUNTER (OTC) ISSUES: Please check all products used regular or occasionally. __pain reliever __ibuprofen (eg. Motrin)
__other: ___________________________________ __Nutritional/Natural Supplements: Pls identify and list products you are using: -herbs, vitamins, minerals, supplements, enzymes, others 6) MEDICAL CONDITIONS/DISEASES. Please check all that apply to you.
__heart disease
__other: _______________________________________________________________________________
7) PRESCRIPTION MEDICATION: List all prescription medication you are using (include physician samples)
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
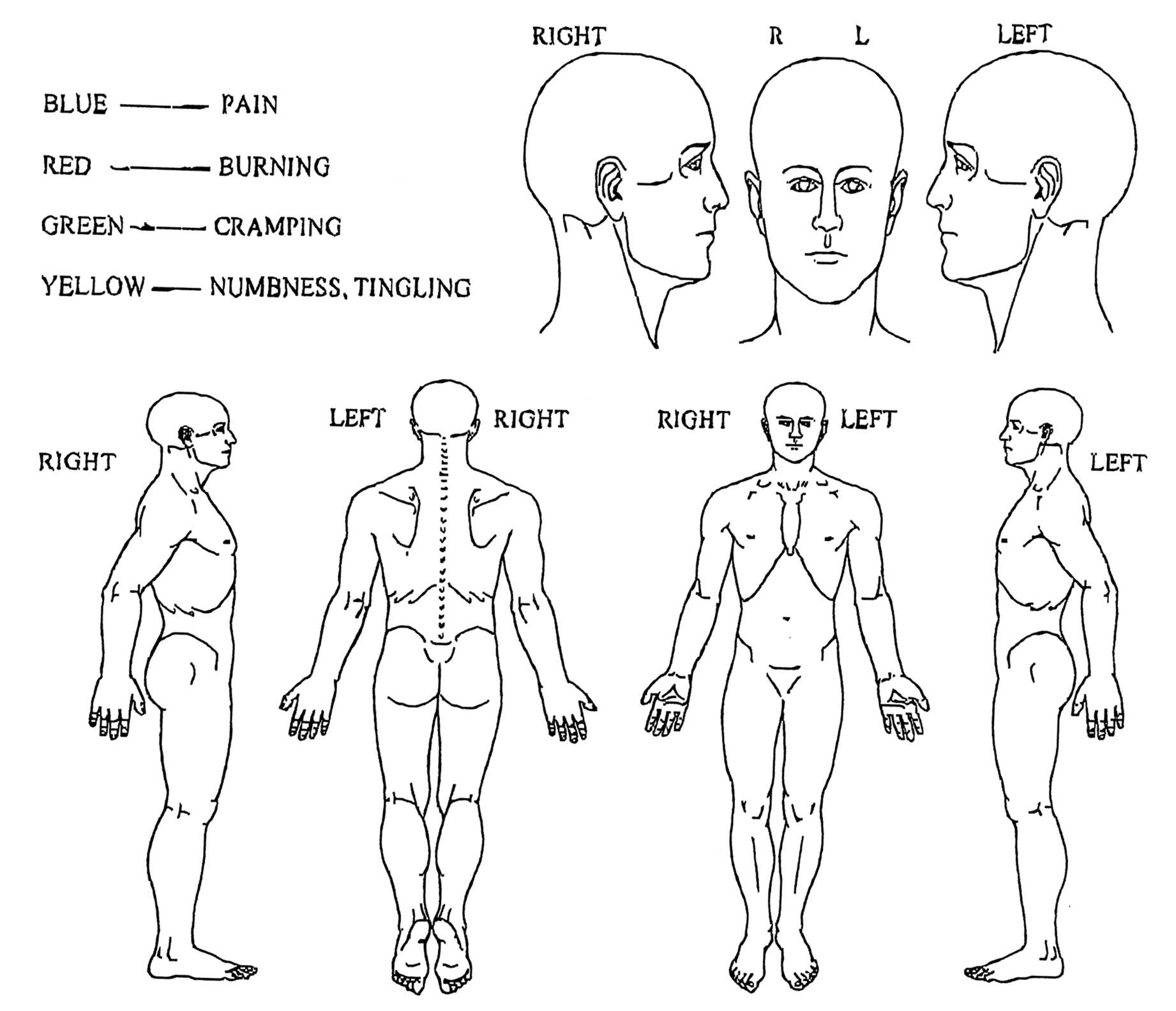
NAME__________________________________________________________DATE_________________ Circle the number that best describes your pain, 0 is NO PAIN and 10 is WORST IMAGINABLE PAIN.
Circle the number that best describes your pain at its worst during the last month.
Circle the number that best describes your pain at its least during the last month.
Circle the number that best describes your pain on average during the last month.
Circle the number that best describes your pain as it is right now.
Only for the use of a Registered Medical Practitioner or a Hospital or a Laboratory. Metformin Hydrochloride and Voglibose Tablets METADOZE V- 0.2/0.3 METADOZE V - 0.2 Distribution: COMPOSITION After ingestion of voglibose (and other glucosidase inhibitors), the majority of active Each uncoated bi-layered tablet contains unchanged drug remains in the lumen of the gastrointestinal t
P A U L - A N D R É B E M P É C H A T C U R R I C U L U M V I T A E Education D.M.A. (Piano/Musicology), Boston University, 2000 - Dissertation: The Life and Works of Jean Cras (1879-1932) - Professors: Isabelle Cazeaux, John Daverio, Musicology Diplôme d’études approfondies (Comparative Literature/Musicology) - Professors: Marie-Claire Beltrando-Patier, Musicology; P

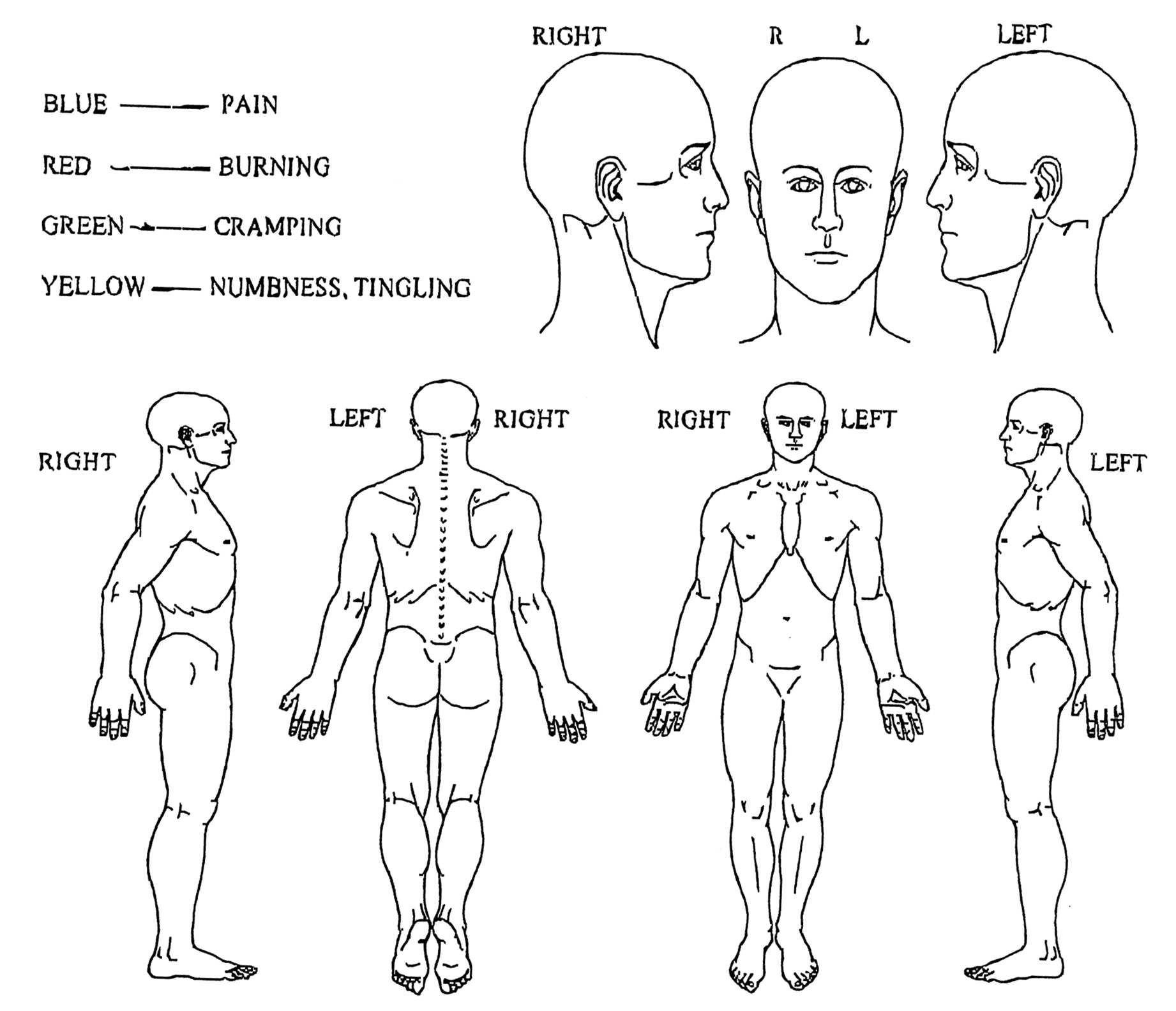
 NAME__________________________________________________________DATE_________________ Circle the number that best describes your pain, 0 is NO PAIN and 10 is WORST IMAGINABLE PAIN.
Circle the number that best describes your pain at its worst during the last month.
Circle the number that best describes your pain at its least during the last month.
Circle the number that best describes your pain on average during the last month.
Circle the number that best describes your pain as it is right now.
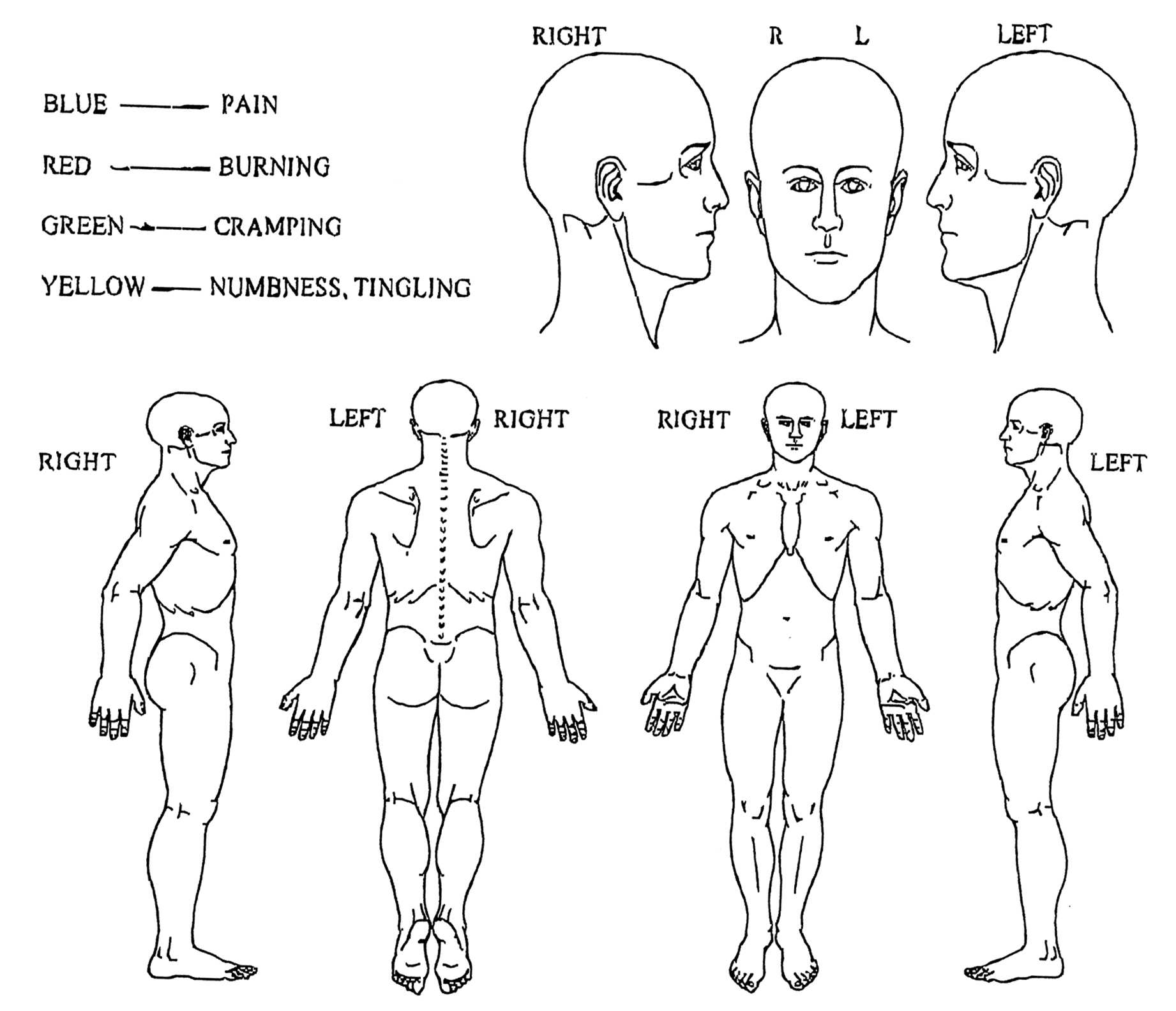
NAME__________________________________________________________DATE_________________ Circle the number that best describes your pain, 0 is NO PAIN and 10 is WORST IMAGINABLE PAIN.
Circle the number that best describes your pain at its worst during the last month.
Circle the number that best describes your pain at its least during the last month.
Circle the number that best describes your pain on average during the last month.
Circle the number that best describes your pain as it is right now.