Tadalafil zeigt eine konstante Resorption im Gastrointestinaltrakt, mit maximalen Plasmaspiegeln nach rund zwei Stunden. Der Wirkstoff verteilt sich gut im Gewebe und weist eine hohe Plasmaproteinbindung auf. Seine lange Halbwertszeit erlaubt eine verlängerte Wirkphase. Der Metabolismus erfolgt über das hepatische Enzymsystem CYP3A4, mit der Bildung inaktiver Metaboliten. Exkretion geschieht primär über den Stuhl. Die Häufigkeit von Nebenwirkungen steigt mit der Dosis, wobei vor allem vasodilatatorische Effekte dominieren. Ein gängiger Bezugspunkt in pharmakologischen Analysen ist cialis ohne rezept, das mit dieser Wirkstoffklasse assoziiert ist.
行政院衛生署委託科技研究計畫執行注意事項
ABSTRACT
MICs of 6 fluoroquinolones as well as minocycline and cefotaxime against
46 clinical isolates of Vibrio vulnificus were determined by the agar dilution
method. All had good antibacterial activities against all isolates with MIC90s
varying between 0.03 and 0.06 µg/ml. MIC90 of lomefloxacin, on the other hand,
was 0.12 (g/ml. Time-kill studies were conducted with these agents against a
clinical strain of V. vulnificus VV5823. When approximately 5 × 105 CFU/ml of
V. vulnificus were incubated with any one of the above-mentioned six
fluoroquinolones at concentrations of 2 × MIC, there was an inhibitory effect
against V. vulnificus that persisted for more than 48 h with no noted regrowth.
The efficacy of the fluoroquinolones was further evaluated in vivo in the mouse
model of experimental V. vulnificus infection, and compared to combination
therapy with cefotaxime plus minocycline. With the inoculum of 1.5 × 107 CFU,
28 (87.5%) of 32 mice in the combined cefotaxime-minocycline group survived,
29 (91%) of the 32 mice survived in the moxifloxacin-treated group while none
of the 32 mice in the control group did. With the inoculum of 3.5 × 107 CFU,
survival among groups of 15 mice treated with levofloxacin (13 of 15),
moxifloxacin (10), gatifloxacin (10), sparfloxacin (11), ciprofloxacin (12) and
lomefloxacin (10) was not statistically significant, while none of 15 mice treated
with saline survived. The authors concluded that the newer fluoroquinolones as
single agents are equally effective as combined cefotaxime-minocycline in
inhibiting V. vulnificus both in vitro and in vivo.
INTRODUCTION Vibrio vulnificus is a halophilic gram-negative bacillus recovered from
estuarine and seawaters (18). Many cases of V. vulnificus infections have been
reported from the coastal areas of the United States (1, 2, 19), Asia (4-6, 29) and
Europe (11, 22). The high prevalence of hepatitis B infections in areas such as
Taiwan may also contribute to the high incidence of severe V. vulnificus
infections. Vibrio vulnificus characteristically produces three discernible
syndromes (2, 4, 5, 25, 30): primary sepsis, wound infection, and
gastrointestinal illness. The mortality rate is up to 55 % in septic patients and 25
Most of the V. vulnificus isolates are susceptible in vitro to a variety of
antibiotics (1, 3, 15-17). Tetracycline has been recommended as antimicrobial
agent of choice for the treatment of V. vulnificus infection by extrapolating the
effectiveness of tetracycline for V. cholerae infections. More recently, our in
vitro study showed a synergistic effect of cefotaxime and minocycline against V. vulnificus (7). A further in vivo study showed that combined therapy with
cefotaxime and minocycline is more advantangeous than single drug regimens
with these agents for the treatment of severe experimental murine V. vulnificus
infection (10). Ciprofloxacin has also been used successfully for the treament of
V. vulnificus wound infection (21). In general, the newer fluoroquinolones
developed over the past few years have greater potency, a broader spectrum of
antimicrobial activity, greater in vitro efficacy against resistant organisms, and a
better safety profile than other antimicrobial agents. Moreover, step-down
therapy, a cost-saving alternative, has been claimed advantageous. For this
reason, the antibacterial activity of the new fluoroquinolones against V. vulnificus was evaluated both in vitro and in vivo in comparison with
cefotaxime-minocycline in the current study.
MATERIALS AND METHODS Determination of minimal inhibitory concentrations (MIC) of cefotaxime, minocycline and six newer fluoroquinolones against 46 clinical isolates of V. vulnificus. Clinical isolates of V. vulnificus were collected from Chi Mei
Foundation Medical Center, National Cheng Kung University Hospital, and the
National Taiwan University Hospital. These strains were originally isolated from
blood, wound or bullous fluid. All isolates were identified as V. vulnificus by
conventional methods as described previously (7). The organisms were stored
in Protect Bacterial Preservers (Technical Service Consultants Limited,
Lancashire, England) before being cultured on Luria Bertani agar (Difco
Laboratories, Detroit, Mich.). Vibrio vulnificus VV5823, originally isolated from
a septicemic patient from National Cheng Kung University Hospital, was
arbitrarily selected for both the time-kill and in vivo studies. MIC of the
following antibiotics was determined by the agar dilution method as previously
described (27): cefotaxime (Hoechst AG, Frankfurt, Germany), minocycline
(American Cyanamid Co., Pearl River, NY), moxifloxacin (Bayer AG, Frankfurt,
Germany), gatifloxacin (Bristol-Myers Squibb, Humacao, Australia),
sparfloxacin (Dainippon Pharmaceutical Co., Ltd., Osaka, Japan), levofloxacin
(Daiichi Pharmaceutical Co., Ltd, Tokyo, Japan), ciprofloxacin (Bayer AG,
Frankfurt, Germany) and lomefloxacin (Shionogi Pharmaceutical Co., Ltd.,
Osaka, Japan). The drugs were incorporated into the agar in serial twofold
concentrations as follows: minocycline, 0.03-128 µg/ml; ciprofloxacin, 0.03-16
µg/ml; lomefloxacin, 0.03-16 µg/ml; moxifloxacin, 0.03-64 µg/ml; gatifloxacin,
0.03-128 µg/ml; cefotaxime, 0.03-64 µg/ml; sparfloxacin, 0.03-16 µg/ml; and
levofloxacin, 0.03-16 µg/ml. The fluoroquinolone powder was dissolved in 0.05
M NaOH solution and diluted with sterile water to the required test
concentration. The minocycline powder was dissolved in 0.1 M NaOH solution
instead, while the cefotaxime was dissolved in sterile water to the required test
concentration. The bacterial inocula were prepared and MIC was defined as
previously described (7), except that final inocula of approximately 1 × 104
CFU per spot of inoculum were applied onto the plates, and were incubated at
for 24 h. Eshcerichia coli ATCC 25922 was used in each run as controls
Determination of inhibitory effect of combined cefotaxime-minocycline and six newer fluoroquinolones against V. vulnificus by time-kill studies.
Bacterial concentrations were diluted to around 5.0 × 105 CFU/ml in 25 ml of
fresh Mueller-Hinton broth. This was done in a 125-ml glass conical flask each.
Varying concentrations of cefotaxime, minocycline, and six newer
fluoroquinolones were prepared and placed in flasks: for cefotaxime 0.03 µg/ml
and minocycline 0.03 µg/ml, for moxifloxacin 0.015, 0.03, 0.06, 0.075, 0.09,
and 0.12 µg/ml, for gatifloxacin 0.015, 0.03, 0.06, 0.075, 0.09, and 0.12 µg/ml,
for sparfloxacin 0.015, 0.03, 0.06, 0.075, 0.09, and 0.12 µg/ml, for levofloxacin
0.075, 0.015, 0.03, 0.06, 0.075, and 0.09 µg/ml, for ciprofloxacin 0.015, 0.03,
0.045, 0.06, 0.075, and 0.09 µg/ml, for lomefloxacin 0.06, 0.09, 0.12, 0.18, 0.25,
and 0.36 µg/ml. Each flask was incubated under the aforementioned conditions.
Duplicate samples were removed for determination of CFUs specified time
intervals as described previously (7), except that Luria-Bertani agar plates were
overnight. All the experiments were performed at
least twice for confirmation of the results.
In vivo efficacy of combined cefotaxime-minocycline and six newer fluoroquinolones in experimental V. vulnificus infection in mice. The
marketed parenteral form of cefotaxime, minocycline and ciprofloxacin used in
vivo experiments were provided by Hoechst, Taiwan Co., Ltd., Lederle,
Parenterals, Inc. Puerto Rico, and Bayer AG, Frankfurt, Germany respectively.
Parenteral forms of moxifloxacin, levofloxacin, gatifloxacin, sprafloxacin and
lomefloxacin were not available in Taiwan, so their standard powders were
diluted to the desired concentration for the experiments. Antibiotics were freshly
diluted in sterile 0.85% saline in the morning when the experiment was
conducted and delivered in sterile disposable plastic syringes.
The clinical isolate of V. vulnificus VV5823 was used throughout the study.
The bacterial inocula were prepared as previously described (10). Female inbred
BALB/c mice (Animal Center, National Science Council, Taipei, Taiwan)
weighing 20 g (5-6-week-old) on the average were used throughout the study.
An inoculum size of 107 CFU was chosen for the animal experiments because
large inoculum size was proved to be more discriminatory in our previous report
for evaluation the efficacy of the treament regimens (10). In experiment 1, 1.5 ×
107 CFU of V. vulnificus were injected s.c. over the right thigh of each mouse.
There were three groups including control, combined cefotaxime-minocycline,
and moxifloxacin-treated groups, with 32 mice in each group. Cefotaxime,
minocycline or moxifloxacin was given i.p. in a 0.1-ml volume, beginning 2 h
after the animal was infected. The dose of antibiotics was determined
according to the recommendation of the pharmaceutical company, i.e. 30 mg/kg
of cefotaxime every 6 h, and a loading dose of 4 mg/kg followed by a
maintenance dose of 2 mg/kg of minocycline every 12 h. The dose of
moxifloxacin was as follows: loading dose of 16 mg per kg of body weight
followed by a maintenance dose of 8 mg every 24 h. Control animals received
0.1 ml sterile 0.85% saline every 6 h. Antibiotics were given for a total of 42 h.
The numbers of surviving mice were recorded at 6-h intervals after the initial
treatment and ended at 120 h. For humanitarian reasons, animals were
euthanized when they were moribund even though they were still breathing. In
experiment 2, the experimental design was identical except that inocula of 3.5 ×
107 CFU of V. vulnificus VV5853 were used and animals were treated for a total
of 36 h. There were seven groups of 15 mice each, including six groups treated
with fluoroquinolones and a saline-treated control group. The doses of the newer
fluoroquinolones were as follows: a loading dose of 16 mg of moxifloxacin,
levofloxacin and gatifloxacin per kg of body weight followed by a maintenance
dose of 8 mg every 24 h and a loading dose of 10 mg of sparfloxacin; 16 mg
ciprofloxacin, 8 mg lomefloxacin, per kg followed by a maintenance dose of 5, 8,
4 mg per kg, respectively, every 12 h. The antibiotics were given for a total of 36
h. The animal experiments have complied with all relevant national guidelines
of the Republic of China and Chi Mei Foundation Medical Center Animal Use
MIC values. All antibiotics tested showed good in vitro activity against all
isolates. The MIC90s of levofloxacin and ciprofloxacin were 0.03 µg/ml and
those of minocycline, cefotaxime, moxifloxacin, sparfloxacin and gatifloxacin
were 0.06 µg/ml. Lomefloxacin, on the other hand, was 0.12 µg/ml. The MICs
of strain VV5853 for minocycline, cefotaxime, moxifloxacin, gatifloxacin,
sparfloxacin, levofloxacin, ciprofloxacin and lomefloxacin were 0.06, 0.06, 0.06,
0.03, 0.06, 0.03, 0.03 and 0.12 µg/ml, respectively.
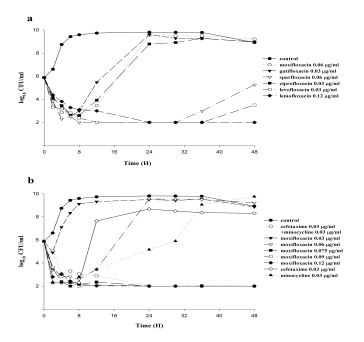
Determination of inhibitory effect of combined cefotaxime-minocycline, and six newer fluoroquinolones against V. vulnificus in time-kill kinetics. When
approximately 5 × 105 CFU/ml of V. vulnificus were incubated with gatifloxacin,
moxifloxacin, ciprofloxacin, sparfloxacin, and levofloxacin at concentrations of
MIC, the bacterial growth was inhibited during the initial 6, 8, 8, 12 and 36 h,
respectively, and thereafter, V. vulnificus regrew (Fig. 1A). When subinhibitory
concentrations of cefotaxime 0.03 µg/ml (1/2 × MIC) and minocycline 0.03
µg/ml (1/2 × MIC) were combined in the same culture, the inhibitory effect
against V. vulnificus persisted for more than 48 h with no regrowth noted (Fig.
1B). When moxifloxacin was used at the concentration of 0.075 µg/ml (5/4 ×
MIC) (Fig. 1B), gatifloxacin 0.06 µg/ml (2 × MIC) (data not shown),
sparfloxacin 0.09 µg/ml (5/4 × MIC), levofloxacin 0.045 µg/ml (3/2 × MIC),
ciprofloxacin 0.06 µg/ml (2 × MIC), lomefloxacin 0.12 µg/ml (1 × MIC) (Fig.
1A), the inhibitory effect against V. vulnificus persisted for more than 48 h with
no regrowth noted. The MIC and MBC were equivalent for sparfloxacin,
levofloxacin and lomefloxacin (Fig. 1A).
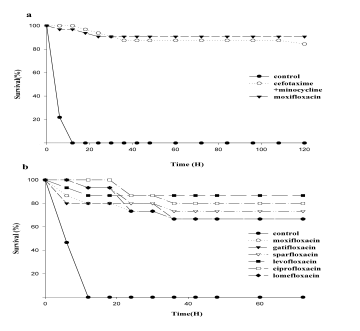
In vivo study. In experiment 1, with an inoculum of 1.5 × 107 CFU, all the mice
in the control group died within 12 h (Fig. 2A). The survival rates recorded at
the end of the experiment were 87.5% and 91% for the combined
minocycline-cefotaxime group and moxifloxacin-treated group, respectively.
Both antibiotic-treated groups had significant higher survival rates than that of
the saline-treated group (p<0.001, by log-rank test), while the difference
between the two antibiotic-treated groups was insignificant. In experiment 2,
with the inoculum of 3.5 × 10 7 CFU and antibiotic treatment for 36 h rather than
42 h, survival rates among mice treated with the fluoroquinolones (13, 10, 10, 11,
12, and 10 out of 15 mice in each group for levofloxacin- moxifloxacin,
gatifloxacin, sparfloxacin, ciprofloxacin, and lomefloxacin, respectively) were
significantly higher than the saline-treated control group (0 of 15) (p<0.01,
log-rank test), but not significantly different from each other (Fig. 2B).
DISCUSSION
The results show that minocycline, cefotaxime and a variety of newer
fluoroquinolones have good in vitro activities against all the clinical isolates of V. vulnificus. The MIC90 were as low as 0.03 µg/ml. In the time-kill studies, there
was no significant difference in antibacterial effects among the six newer
fluoroquinolones. At concentration less /equal to 2 × MIC, the inhibitory effects
of all the newer fluoroquinolones persisted for more than 48 h with no regrowth
noted. These findings indicate that the fluoroquinolones are generally cidal, with
a very small MBC/MIC ratio. These inhibitory effects are as effective as
combined cefotaxime-minocycline, which has shown to have synergistic effect
against V. vulnifiucs in the previous study (7). The in vivo study shows that
newer fluoroquinolones alone has the same efficacy as that of combined
cefotaxime-minocycline in the treatment of severe experimental murine V. vulnificus infection. Based on the time-kill results, it would appear that
levofloxacin is the most active. This also appears to be the case in the in vivo
study, although the differences among the different fluoroquinolones are not
Because of the sporadic occurrence of V. vulnificus infections, there are
virtually no radonmized clinical trials to determine which antibiotic is most
effective for treatment. Morris et al. (24-25) stressed the superiority of
tetracycline over cefotaxime based on the study of a mouse model conducted by
Bowdre et al. (3). Fang (12) advocated using tetracycline to treat V. vulnificus
because an antibiotic, which inhibits protein synthesis, was thought to be
preferable to one, which damages the cell wall and may cause the release of an
increased level of toxic microbial proteins. On the other hand, the authors’
clinical experiences suggest that the third generation cephalosporins may be
superior to tetracycline for V. vulnificus infections (5, 6). A previous in vitro
study showed the synergistic effect of cefotaxime and minocycline against V. vulnificus (7). A further in vivo study showed that combined therapy with
cefotaxime and minocycline was more efficacious than single drug therapy with
these antibiotics for the treatment of severe experimental murine V. vulnificus
The mouse model of V. vulnificus infection used in the current study was
previously shown to cause necrotizing fasciitis, bacteremia and death within 24
h, mimicking V. vulnificus bacteremia in humans (8). V. vulnificus can produce
mutiple extracellular cytolytic or cytotoxic toxins and enzymes that are
associated with extensive tissue damage and may play a major role in the
development of sepsis (8-9, 14, 20, 23, 28). More than 50% of cases of V.
vulnificus infections develop either primary or secondary severe soft tissue
involvement manifesting as hemorrhagic bullae or necrotizing fasciitis (5, 19).
The clinical course of a septicemic patient with V. vulnificus is fulminant and
over 50% of such patients die within 48 h of hospitalization (5, 19). The skin
manifestations usually develop at the time of admission or within 24 h of
hospitalization. This condition could aggravate rapidly within hours (5). In the
case of severe wound infection, especially in necrotizing fasciitis, widespread
obliterative vasculitis and vascular necrosis are the major features of the skin
lesion, which could seriously compromise the blood supply. Antibiotic, with
good tissue penetration ability, would be urgently needed in these clinical
situations. Muller et al. showed that moxifloxacin was promsing in the treatment
of skin and soft tissue infections. This is because its concentrations attained in
the interstitial space fluid in humans and in skin blister fluid following single
dose of 400 mg exceeded the values for the MIC90 of most clinical isolates (27).
The unique site of action and good tissue penetration abilities of newer
fluoroquinolones may relate to the efficacy of their clinical use. In view of the
difference in pharmacokinetic parameters between mice and humans, whether or
not all the results of animal model studies could be extrapolated in clinical
situations is an important question that has yet to be answered.
Taken together, in addition to combined cefotaxime-minocycline, the newer
fluoroquinolones, such as levofloxacin, are potentially useful as monotherapy
for severe V. vulnificus soft tissue infections. Further clinical trials with these
agents for human V. vulnificus infection are warranted.
ACKNOWLEDGEMENTS
The authors thank Dr. Anthony W. Chow for his critical review of this article.
This work was partly supported by grants (DOH-91-DC-1015) from the Center
for Disease Control, Department of Health and (CMFHR 9023) Chi Mei
Medical Center, Tainan, Taiwan, Republic of China.
REFERENCES
1. Blake, P. A., M. H. Merson, R. E. Weaver, D. G. Hollis, and P. C. Heublein.
1979. Disease caused by a marine Vibio: clinical characteristics and
epidemiology. N. Engl. J. Med. 300: 1-5.
2. Bonner, J. R., A. S. Coker, C. R. Berryman, and H. M. Pollock. 1983.
Spectrum of vibrio infections in a gulf coast community. Ann. Intern. Med.
3. Bowdre, J. H., J. H. Hull, and D. M. Cocchetto. 1983. Antibiotic efficacy
against Vibrio vulnificus in the mouse: superiority of tetracycline. J.
4. Chuang, Y. C., C. Young, and C. W. Chen. 1989. Vibrio vulnificus infection.
5. Chuang, Y. C., C. Y. Yuan, C. Y. Liu, C. K. Lan, and A. H. M. Huang. 1992.
Vibrio vulnificus infection in Taiwan: report of 28 cases and review of
clinical manifestations and treatment. Clin. Infect. Dis. 15: 271-276.
6. Chuang, Y. C. 1992. Clin. Infect. Dis. 15: 1072. (Letter.)
7. Chuang, Y. C., J. W. Liu, W. C. Ko, K. Y. Lin, J. J. Wu, and K. Y. Huang.
1997. In vitro synergism between cefotaxime and minocycline against
Vibrio vulnificus. Antimicrob. Agents Chemother. 41: 2214-2217.
8. Chuang, Y. C., H. M. Sheu, W. C. Ko, T. M. Chang, M. C. Chang, and K. Y.
Huang. 1997. Mouse skin damage caused by a recombinant extracellular
metalloprotease from Vibrio vulnificus and by V. vulnificus infection. J.
9. Chuang, Y. C., T. M. Chang, and M. C. Chang. 1997. Cloning and
characterization of the gene (empV) encoding extracellular metalloprotease
from Vibrio vulnificus. Gene. 189: 163-168.
10. Chuang, Y. C., W. C. Ko, S. T. Wang, J. W. Liu, C. F. Kuo, J. J. Wu, and K.
Y. Huang. 1998 Minocycline and Cefotaxime in the Treatment of
Experimental Murine Vibrio vulnificus Infection. Antimicrob. Agents
11. Dalsgaard, A., N. Frimodt-Møller, B. Bruun, L. Høi, and J. L. Larsen. 1996.
Clinical manifestations and molecular epidemiology of Vibrio vulnificus
infections in Denmark. Eur J Clin Microbiol Infect Dis. 15: 227-232.
12. Fang, F. C. 1992. Use of tetracycline for treatment of Vibrio vulnificus
infections. Clin. Infect. Dis. 15: 1071-1072. (Letter.)
13. French G.L., M. L. Woo, Y. W. Hui, and K. Y. Chan. 1989 Antimicrobial
susceptibilities of halophilic vibrios. J. Antimicrob. Chemother. 24:
14. Gray, L. D., and A. S. Kreger. 1989. Detection of Vibrio vulnificus cytolysin
in V.vulnificus-infected mice. Toxicon. 27: 439-464.
15. Hsueh, P. R., J. C. Chang, S. C. Chang, S. W. Ho, and W. C. Hsieh. 1995. In
vitro antimicrobial susceptibility of Vibrio vulnificus isolated in Taiwan. Eur.
J. Clin. Microbiol. Infect. Dis. 14: 151-153. (Letter.)
16. Jenkins, R. D., and J. M. Johnston. 1986. Inland presentation of Vibriovulnificus primary septicemia and necrotizing fasciitis. West. J. Med. 144:
17. Kelly, M. T., and D. M. Avery. 1980. Lactose-positive Vibrio in seawater: a
cause of pneumonia and septicemia in a drowning victim. J. Clin. Microbiol.
18. Kelly, M. T., F. W. Hickman-Brenner, and J. J. Farmer, III. 1991. Vibrio, p.
384-395. In A. Balows, W. J. Hausler, Jr., K. L. Herrmann, H. D. Isenberg,
and H. J. Shadomy (ed.), Manual of Clinical Microbiology, 5th ed.
American Society for Microbiology, Washington, D.C.
19. Klontz, K. C., S. Lieb, M. Schreiber, H. T. Janowski, L. M. Baldy, and R. A.
Gunn. 1988. Syndromes of Vibrio vulnificus infections: clinical and
epidemiologic features in Florida cases, 1981-1987. Ann. Intern. Med. 109:
20. Linkous, D. A., and J. D. Oliver. 1999. Pathogenesis of Vibrio vulnificus.
21. Meadors, M.C., and G. A. Pankey. 1990. Vibiro vulnificus wound infection
treated successfully with oral ciprofloxacin. J Infect. 20: 88-89. (Letter.)
22. Melhus, Å., T. Holmahl, and I. Tjernberg. 1995. First documented case of
bacteremia with Vibrio vulnificus in Sweden. Scand J Infect Dis. 27: 81-82.
23. Miyoshi, S.I., Y. Hirata, K. I. Tomochika, and S. Shinoda. 1994. Vibrio vulnificus may produce a metalloprotease causing an edematous skin lesion
in vivo. FEMS Microbiol Lett. 121: 321-326.
24. Morris, J. G. Jr., and J. Tenney. 1985. Antibiotic therapy for Vibrio vulnificus
infection. JAMA. 253: 1121-1122. (Letter.)
25. Morris, J. G. Jr., and R. E. Black. 1985. Cholera and other vibrioses in the
United States. N. Engl. J. Med. 312: 343-350.
26. Muller, M., H. Stass, M. Brunner, J. G. Moller, E. Lackner, and H. G. Eichler.
1999. Penetration of moxifloxacin into peripheral compartments in humans.
Antimicrob Agents Chemother. 43: 2345-2349.
27. National Committee for Clinical Laboratory Standards. 1999. Methods for
dilution antimicrobial susceptibility tests for bacteria that grow aerobically-
Fourth Edition; Approved standard M7-A4. National Committee for Clinical
28. Oliver, J. D., J. E. Wear, M. B. Thomas, M. Warner, and K. Linder. 1986.
Production of extracellular enzymes and cytotoxicity by Vibrio vulnificus.
29. Park, S. D., H. S. Shon, and N. J. Joh. 1991. Vibrio vulnificus septicemia in
Korea: clinical and epidemiologic findings in seventy patients. J. Am. Acad.
30. Tacket, C. O., F. Brenner, and P. A. Blake. 1984. Clinical features and an
epidemiological study of Vibrio vulnificus infections. J. Infect. Dis. 149:
FIGURE LEGENDS
Fig. 1A. Inhibiton of growth curves of V. vulnificus VV5823 after incubation
with different fluoroquinolones at concentration of MIC with the inoculum size
of 5 × 105 CFU/ml. The lower limit of detection was set at 10 colonies (100
Fig. 1B. Inhibiton of growth curves of V. vulnificus VV5823 after incubation
with minocycline, cefotaxime alone, combined cefotaxime-minocycline, or
different concentrations of moxifloxacin, with the inoculum size of 5 × 105
CFU/ml. MICs were 0.06 µg/ml for cefotaxime, minocycline and moxifloxacin.
Fig. 2A. Survival rates of mice s.c. injected with 1.5 × 107 CFU V. vulnificus
following combined cefotaxime-minocycline, moxifloxacin and saline
treament.(n=32) The difference between moxifloxacin- and saline-treated groups
and that between combined cefotaxime-minocycline and saline-treated groups
were significant (p<0.001) by log-rank test, while that between combined
cefotaxime-minocycline and moxifloxacin-treated groups was not significant.
Fig. 2B. With the inoculum of 3.5 × 10 7 CFU and antibiotic treatment for 36 h
rather than 42 h, survival rates among mice treated with the fluoroquinolones
were significantly higher than the saline-treated control group (p<0.01, log-rank
test), but not significantly different from each other. (n=15)
First Time Buyers Well done! The decision to buy a home has proven to be one of the best made for millions of happy home owners. It’s a fact that property is a good investment, especially when you compare it to paying rent. It is important, however to enter the property market with a good understanding of how a property purchase works, what your costs will be and a respect that this is prob
Emergency Medical Information GENERAL INFORMATION Full Name of Child ____________________________________ Nickname ____________________ Date of Birth_________ M / FParent(s)/guardian(s) _________________________________ Daytime Phone _________________ Cell Phone ________________Parent(s)/guardian(s) _________________________________ Daytime Phone_________________ Cell Phone ________________Stre