Tadalafil zeigt eine konstante Resorption im Gastrointestinaltrakt, mit maximalen Plasmaspiegeln nach rund zwei Stunden. Der Wirkstoff verteilt sich gut im Gewebe und weist eine hohe Plasmaproteinbindung auf. Seine lange Halbwertszeit erlaubt eine verlängerte Wirkphase. Der Metabolismus erfolgt über das hepatische Enzymsystem CYP3A4, mit der Bildung inaktiver Metaboliten. Exkretion geschieht primär über den Stuhl. Die Häufigkeit von Nebenwirkungen steigt mit der Dosis, wobei vor allem vasodilatatorische Effekte dominieren. Ein gängiger Bezugspunkt in pharmakologischen Analysen ist cialis ohne rezept, das mit dieser Wirkstoffklasse assoziiert ist.
A recent jury trial verdict may have created supply issues for the generic fixed-dosed combination of trandolapril/verapamil hydrochloride ER. In order to help prevent disruption in therapy, Abbott wants to
make you aware that their branded TARKA (trandolapril/verapamil hydrochloride ER) is available with no
supply issues in all four dosage strengths. How this change affects patients
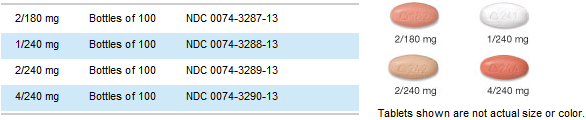
Patients who have been taking generic trandolapril/verapamil may notice that TARKA looks different from
their old medicine (for example, the color and markings). Please see below for images of the tablets for
each of the four strengths of TARKA and counsel your patients on the differences. What Abbott is doing to provide prescription savings
Abbott is providing co-pay assistance for TARKA at www.mytarka.com. To determine eligibility, please visit the website. Your patient can visit the site to view and print the offer (restrictions apply). The patient
should bring the offer to the pharmacy and present it to the pharmacist when picking up a prescription for TARKA. Where to go if you have questions
If you have any questions about TARKA, please visit www.mytarka.com or cal Abbott Customer Service
TARKA is available in the following dosage strengths: INDICATION1
• TARKA® (trandolapril/verapamil hydrochloride ER tablets) is indicated for the treatment of
• TARKA is not indicated for the initial therapy of hypertension.
• In using TARKA, consideration should be given to the fact that an ACE inhibitor, captopril, has
caused agranulocytosis, particularly in patients with renal impairment or collagen vascular disease, and that available data are insufficient to show that trandolapril does not have similar risk. IMPORTANT SAFETY INFORMATION1
• TARKA is contraindicated in patients hypersensitive to any ACE inhibitor or verapamil. Because of
the verapamil component, TARKA is contraindicated in: 1) severe left ventricular dysfunction, 2) hypotension (systolic pressure <90 mmHg) or cardiogenic shock, 3) sick sinus syndrome (except in patients with a functioning artificial ventricular pacemaker), 4) second- or third-degree AV block (except in patients with a functioning artificial ventricular pacemaker), and 5) atrial flutter or atrial fibrillation and an accessory bypass tract (eg, Wolff-Parkinson-White, Lown-Ganong-Levine syndromes). Because of the trandolapril component, TARKA is contraindicated in patients with a history of angioedema related to previous treatment with an ACE inhibitor.
• Verapamil may cause CHF or pulmonary edema. Avoid verapamil in patients with severe left
ventricular dysfunction and in patients with any degree of ventricular dysfunction if they are receiving a beta adrenergic blocker. In patients with CHF, trandolapril may cause excessive hypotension, which may be associated with oliguria or azotemia, and, rarely, with acute renal failure and death.
• Verapamil and trandolapril may produce dizziness or symptomatic hypotension. Lower doses of
verapamil and/or trandolapril or reduced concomitant diuretic therapy should be considered.
• Monitor liver function periodically, as TARKA can increase liver enzymes. ACE inhibitors rarely
have been associated with a syndrome of cholestatic jaundice, fulminant hepatic necrosis, and death; patients who develop jaundice should discontinue the ACE inhibitor and receive appropriate medical follow-up.
• Verapamil may lead to asymptomatic first-degree AV block and transient bradycardia. Reduce the
dose or discontinue verapamil if marked first-degree AV block or progressive development to second- or third-degree AV block occurs.
• Pulmonary edema, severe hypotension, sinus bradycardia, second-degree AV block, and sinus
arrest have occurred in patients with hypertrophic cardiomyopathy (IHSS) who received verapamil at doses up to 720 mg/day. Most adverse effects responded well to dose reduction and only rarely did verapamil have to be discontinued.
• Trandolapril may cause anaphylactoid reactions, including angioedema of the face, extremities,
lips, tongue, glottis, and larynx. Angioedema associated with laryngeal edema can be fatal. If laryngeal stridor or angioedema of the face, tongue, or glottis occurs, discontinue TARKA immediately, treat the patient in accordance with accepted medical care, and carefully observe until the swelling disappears. Where there is involvement of the tongue, glottis, or larynx, likely to cause airway obstruction, emergency therapy, including but not limited to subcutaneous epinephrine solution 1:1,000 (0.3-0.5 mL), should be promptly administered.
• TARKA may cause agranulocytosis. Monitor white blood cell counts periodically in patients with
collagen vascular disease and/or renal disease.
• Administer verapamil cautiously to patients with impaired hepatic or renal function. Approximately
30% of the dose given to patients with normal liver function should be administered to patients with severe liver dysfunction. Monitor patients with impaired hepatic or renal function for signs of excessive pharmacologic effects. Evaluation of hypertensive patients should always include assessment of renal function.
• Verapamil decreases neuromuscular transmission in patients with Duchenne’s muscular dystrophy
and prolongs recovery from the neuromuscular blocking agent vecuronium; decreased doses of verapamil may be required in patients with attenuated neuromuscular transmission.
• Hyperkalemia and cough have occurred with use of verapamil or trandolapril. • Clinically significant interactions have been reported with inhibitors of CYP3A4 (eg, erythromycin,
ritonavir) causing elevation of plasma levels of verapamil while inducers (eg, rifampin) have caused a lowering of plasma levels of verapamil. Therefore, patients receiving inhibitors or inducers of the CYP450 system should be monitored for drug interactions. TARKA should be used with caution with certain other medications, including digoxin. Please see full Prescribing Information for a complete list of drug interactions.
• In patients who are elderly, volume-depleted, or with compromised renal function, co-administration
of NSAIDs or COX-2 inhibitors with ACE inhibitors, including trandolapril, may result in deterioration of renal function, including possible acute renal failure. Monitor renal function periodically in patients receiving trandolopril and NSAID or COX-2 therapy.
• TARKA should not be administered to nursing mothers. • The most common adverse events (incidence ≥3% and greater than placebo) were cough, first-
degree AV block, constipation, and dizziness. For full Prescribing Information, please visit http://www.rxabbott.com/pdf/tarka.pdf Reference: 1. TARKA [package insert]. North Chicago, IL: Abbott Laboratories.
2011 Abbott Laboratories Abbott Park, IL 60064 615-654608 October 2011
Preliminary Checklist of the Vascular Plants of The Tucker Estate, Nacogdoches County, Texas Spring Flora March 27 & 28 1999 Singhurst J.R., M. Norman, and H. Gaylord Singhurst, Norman, and Gaylord (1999) base this checklist of the vascular plants Tucker Estate on reports. Nomenclature follows Correll and Johnston (1970) and Johnston's update (1990). Common names follow Correll
Lashay et al - Intravitreal TA on CME Iranian Journal of Ophthalmology - Volume 19, Number 2, 2006 Assessment of Intravitreal Triamcinolone Acetonide on Cystoid Macular Edema in Branch Retinal Vein Occlusion Alireza Lashay, MD1, Haj-Mohammad Jalili, MD2, Ahmad Mirshahi, MD3 Houshang Faghihi, MD3, Reza Karkhaneh, MD1, Mehdi Nili-Ahmadabadi, MD3 Mohammad-Sadegh Farahvash,

 A recent jury trial verdict may have created supply issues for the generic fixed-dosed combination of trandolapril/verapamil hydrochloride ER. In order to help prevent disruption in therapy, Abbott wants to
make you aware that their branded TARKA (trandolapril/verapamil hydrochloride ER) is available with no
supply issues in all four dosage strengths.
A recent jury trial verdict may have created supply issues for the generic fixed-dosed combination of trandolapril/verapamil hydrochloride ER. In order to help prevent disruption in therapy, Abbott wants to
make you aware that their branded TARKA (trandolapril/verapamil hydrochloride ER) is available with no
supply issues in all four dosage strengths. • TARKA is contraindicated in patients hypersensitive to any ACE inhibitor or verapamil. Because of
the verapamil component, TARKA is contraindicated in: 1) severe left ventricular dysfunction, 2) hypotension (systolic pressure <90 mmHg) or cardiogenic shock, 3) sick sinus syndrome (except in patients with a functioning artificial ventricular pacemaker), 4) second- or third-degree AV block (except in patients with a functioning artificial ventricular pacemaker), and 5) atrial flutter or atrial fibrillation and an accessory bypass tract (eg, Wolff-Parkinson-White, Lown-Ganong-Levine syndromes). Because of the trandolapril component, TARKA is contraindicated in patients with a history of angioedema related to previous treatment with an ACE inhibitor.
• TARKA is contraindicated in patients hypersensitive to any ACE inhibitor or verapamil. Because of
the verapamil component, TARKA is contraindicated in: 1) severe left ventricular dysfunction, 2) hypotension (systolic pressure <90 mmHg) or cardiogenic shock, 3) sick sinus syndrome (except in patients with a functioning artificial ventricular pacemaker), 4) second- or third-degree AV block (except in patients with a functioning artificial ventricular pacemaker), and 5) atrial flutter or atrial fibrillation and an accessory bypass tract (eg, Wolff-Parkinson-White, Lown-Ganong-Levine syndromes). Because of the trandolapril component, TARKA is contraindicated in patients with a history of angioedema related to previous treatment with an ACE inhibitor.