Tadalafil zeigt eine konstante Resorption im Gastrointestinaltrakt, mit maximalen Plasmaspiegeln nach rund zwei Stunden. Der Wirkstoff verteilt sich gut im Gewebe und weist eine hohe Plasmaproteinbindung auf. Seine lange Halbwertszeit erlaubt eine verlängerte Wirkphase. Der Metabolismus erfolgt über das hepatische Enzymsystem CYP3A4, mit der Bildung inaktiver Metaboliten. Exkretion geschieht primär über den Stuhl. Die Häufigkeit von Nebenwirkungen steigt mit der Dosis, wobei vor allem vasodilatatorische Effekte dominieren. Ein gängiger Bezugspunkt in pharmakologischen Analysen ist cialis ohne rezept, das mit dieser Wirkstoffklasse assoziiert ist.
Microsoft word - bladder.doc
Bladder management
Spinal cord injury at any level almost always affects your control over your bladder and bowels. This is because the nerves controlling these internal organs are attached to the very base of the spinal cord (levels S2 - 4), and then pass down through the cauda equina, the ‘horse’s tail’ below the cord itself. Although you will not have the same control that you were used to before your injury - a whole range of techniques exist to help you to ‘manage’ your bladder and bowels. These techniques include the use of movement, implanted electrodes and/or drugs to stimulate muscles which no longer respond to your brain; diet and/or drugs to slow down or speed up the way the body handles fluids and solids; the use of tubes and drainage bags; and re-routing of the body’s drainage channels. Each individual is different, but used singly or in combination, appropriate continence aids and techniques should enable you to re-establish a degree of control over both your bladder and bowels. How the bladder works Urine consists of excess water and salts which are extracted from the bloodstream by the kidneys, which continually control the level of these in the blood. From the kidneys the urine is pumped down thin tubes called ureters, which normally allow the urine to flow only in one direction. The ureters are connected to the bladder, a muscular bag in which urine is stored until it is convenient to empty it. Expansion and contraction of the bladder is controlled by the detrusor muscle. When the bladder is full, nerves send a message via the spinal cord to the brain. When you decide to urinate, the brain sends a message down the spinal cord to release the inhibition on the spinal reflex arc. This will allow the detrusor muscle to contract, and the sphincter muscle around the top of the urethra to relax and open. Urine then passes down the urethra to exit via your penis or by your vulva. Reflex activity of the nervous system (where messages are processed within the lower part of the spinal cord, without having to travel all the way to and from the brain) also controls the bladder muscles - a baby doesn’t wet itself continually, but only when its bladder is full enough to trigger the reflex to empty it. Acontractile & reflex bladders After injury, the body’s normal system of bladder control no longer works, because messages can no longer pass between the bladder muscles and the brain. If your injury is T12 or above, you usually have what is called a reflex (or ‘automatic’ or ‘spastic’ bladder). With an injury below the T12 level you will usually have an acontractile (or ‘flaccid’) bladder. Reflex bladder: reflex bladder allows automatic involuntary control of the bladder so that when the bladder fills above a certain level it contracts and urine flows out automatically. The reflex can be triggered by ‘tapping’ (see ‘tapping’). However, a rapid movement, laughter or spasm can trigger bladder emptying when you don’t expect it Acontractile bladder: with lower lesions, the reflex arc is also damaged, the bladder has no muscle tone and doesn’t contract to empty automatically. Instead, it continues to fill and small amounts of urine may eventually dribble out. The bladder can be emptied at regular intervals by intermittent self- catheterisation (see below). The final outcome of how your bladder would behave is not solely related to the level of injury. There may be other factors which will have influence. After injury
Although there have been huge improvements (in 1917 almost half of all people with spinal cord injury died of urinary sepsis within two months), urinary tract (and hence kidney) complications are still one of the main causes of illness and death in spinal cord injured people. So correct bladder management is, literally, vital. In the first few weeks after injury, your bladder will commonly need to be emptied regularly through a fine tube or catheter. This is either inserted every few hours by a nurse through your urethra (the tube through which you void or ‘pee’) and up into the bladder, and then withdrawn when the bladder is empty; or a small surgical incision is made just above your pubic area, and a ‘suprapubic’ catheter inserted directly into your bladder and left in place. After a few weeks you will be gradually trained to empty your own bladder. The method used depends on the level of your lesion, your bladder behaviour and whether you are male or female. Bladder training
Bladder training is a process to teach the individual to manage and to empty their bladder without the need for an instrument. Bladder training depends on your bladder behaviour. Some bladders would require training to become reflex bladders and others would need training as contractile bladders. All methods of bladder management involve a degree of training and routine. In the past some people with spinal cord injury were taught to regularly transfer onto a toilet and to express or ‘bear down’, to expel urine, negating the need for catheters or drainage bags. This method of management is no longer taught at spinal injuries centres as it may result in stress incontinence, and cannot be relied upon as a sole method of bladder management to achieve continence. It is important that your bladder strength and capacity is not reduced by allowing your bladder to remain empty (ie. by indwelling catheter on free drainage). To maintain or increase bladder strength and capacity your bladder is trained to regularly hold a volume of urine. Catheter valve
This is placed between the catheter tube and the urinary drainage bag. The valve has a tap which when turned off stops urine from draining into the bag. Bladder strength and capacity may be improved by gradually increasing the time that the catheter valve tap is turned off. Some spinal cord injured people are able to use a catheter valve without a drainage bag, by opening the valve’s tap over a toilet or into a urinal at regular intervals. Other people use a spigot to stop urinary drainage. Bathing, swimming, wearing shorts or skirts is not a problem as a ‘spigot’ can be put on the end of the tube [of an indwelling catheter] instead of the leg bag. This effectively stops the bladder draining but it can be opened for drainage straight into a toilet. These spigots work excellently, enabling the tube to be just tucked away in a swimsuit or under clothing. I wished these had been made available to me at thesame time I started using the suprapubic catheter, as I feel I would probably have used the leg bag less, and the spigots more. • Jean Ginder, T10/11 complete
Care should be taken when using a catheter valve or spigot if you easily develop autonomic dysreflexia. Warning signs of a full bladder
Training also involves learning to recognise the signs that your bladder needs emptying. These will vary depending on the level of your lesion, but may include backache, abdominal fullness and, in high lesion paraplegics and tetraplegics, headache, sweating, flushing of the face, neck and shoulders and goose pimples. Autonomic dysreflexia
WARNING:In tetraplegics and paraplegics with lesions at T6 or above, an overfull bladder, or a bladder that is generating high pressure during passing water, are the commonest causes of autonomic dysreflexia, a sudden and potentially life-threatening surge in blood pressure. It is vital that you know how to recognise the signs of this and take appropriate action. Fluid intake Given the difficulties with continence, it may be tempting to drink less fluid. This is a mistake, especially if you use an indwelling catheter: you need a good fluid throughput to keep your kidneys clean and bladder washed out and functioning properly. If you are prone to urinary tract infections, then increase your fluid intake (preferably to at least 3 litres or 5 pints per 24 hours), make sure your urine is slightly acid and if necessary take vitamin C (but not the effervescent type) or drink cranberry juice to increase the acidity. Some people also take urinary antiseptics in conjunction with Vitamin C to maximise its effects. Regular emptying
It is essential that your bladder is emptied regularly (preferably every 3–4 hours during waking hours) and as completely as possible. An overfull bladder may cause urine to reflux or ‘back up’ into your kidneys and can cause infection and damage. In tetraplegics it can cause autonomic dysreflexia). Inadequate emptying of the bladder causes sediment and deposits to build up, increasing the likelihood of infection and bladder stones. Toilets
Make sure that your toilet at home is well adapted for you: easy to get in and out of, with hand rails in the right place, a handbasin at a suitable height, a padded toilet seat (important to avoid pressure sores), a low shelf or work surface and the supplies you require within easy reach. If you are able to use one, a bidet can be a godsend. Alternatively, there are special combined toilet/bidets. Take care that the water is not too hot. Catheters
Intermittent self-catheterisation This is often the method of choice for people with acontractile bladders, and is commonly used by men and women with paraplegia. Patients with reflex bladders that have good capacity can also use this method. Anyone with sufficient hand control can learn to self-catheterise, though dexterity is required to insert the catheter without damaging the urethra. You are less likely to get an infection if you change your own catheter than if someone else does it for you. Both men and women can usually catheterise while in bed, in the wheelchair or on the toilet. The aims of intermittent self-catheterisation are to empty your bladder completely at regular intervals, and to achieve continence without the need to wear an appliance. It is important with all catheters not to use too large a size which can damage your urethra. The main disadvantage is that you need some privacy or access to a toilet or bathroom, and you may not be able to rely on this when travelling or away from home. Care with hygiene is required to avoid bladder infections, but the risk is less than with an indwelling catheter. It is important to thoroughly cleanse your hands and genital area before passing the catheter. To insert a catheter, wash your hands and your penis or labia thoroughly with soap and water (if you have no access to these, baby wipes will do, but should not be used too often as they may cause soreness). Men insert gel into the urethra, women dip the tip of the catheter into a blob of gel placed on a clean surface (e.g. a paper towel). Men need to hold the penis up to straighten the urethra. Pass the catheter gently up into the bladder, pausing if resistance is felt. Once urine begins to flow apply gentle pressure to the lower abdomen with the flat or heel of your hand and continue until the urine flow stops.
Gradually withdraw the catheter (1-2cm at a time), stop each time urine begins to flow out and wait until the flow stops before continuing to withdraw the catheter out. Unless you are in the toilet, a plastic bag or small container is needed to collect the urine. There are two types of catheters – plain and lubricated. With plain catheters a separate lubricant is required. A catheter can be reused for up to one week - it should be washed in soap and water, then rinsed and flicked dry. It should be stored in a container of Milton, and the solution changed daily. While you are away from home the catheter can be dried and stored in a clean plastic bag. Lubricated catheters either come packaged in their own solution and are ready for use, or need water (tap water is fine in the UK) added to the packaging to activate the lubricant (this takes 30 seconds). After use the catheter is then disposed of, i.e. single use only. Also available are complete sets of intermittent catheterisation equipment which contain the catheter, lubricant and a collecting bag. These are particularly useful where toilets are not available or suitable, at work, when abroad or during the night. Indwelling urethral catheters Using an indwelling urethral catheter for long term bladder management is best avoided. Long term use can cause urethral dilatation, chronic bladder infection, penis splitting and bladder stones. Sediment and small calcium granules (which grow to form stones) gather around the balloon and can easily block the catheter. Regular bladder instillations may be recommended, with caution, and you should increase your daily intake of fluid to 3.5 litres (6 pints). Many women use one occasionally when travel away from home means that they cannot rely on access to toilets to self-catheterise. The catheter is inserted through the urethra in the usual way, but kept permanently in place by a small balloon on the end inside the bladder. Once the catheter has been inserted, the balloon is inflated with sterile water, and expands to hold the catheter in place. Indwelling urethral catheters need to be changed regularly, every 4-6 weeks. If you have sufficient hand control (and not too much spasm) you should be able to change your own. Otherwise your personal assistant or district nurse will need to do it. Great care needs to be taken to ensure that the catheter itself and everything used in the changing process are sterile. There is a high risk of infection as an indwelling catheter leaves the urinary tract permanently ‘open’ for bacteria to enter. You may be advised to use a catheter valve and to close this for 3–4 hours at a time to ensure that your bladder fills regularly and doesn’t get ‘lazy’. To remove: a syringe is inserted into the side entrance of the catheter and the balloon is deflated by allowing the sterile water to drain into the syringe. This should happen without the need to ‘pull back’ on the syringe. However, if you have difficulty deflating the balloon, leave the syringe in place for al minute before applying gentle suction. If this fails, seek help from a doctor or hospital. Never apply force or cut any part of the catheter. Indwelling catheter Male Female
To insert: 1. place a sterile paper sheet over the abdomen with a hole cut out in the appropriate place. 2. place a sterile swab around the penis or between the labia. 3. thoroughly swab the glands of the penis, or the labia with an antiseptic wash. 4. men insert lubricant gel into the urethra or onto the catheter, and hold the penis up to straighten the
5. women put a blob of lubricant gel on a paper towel and dip in the tip of the catheter just before
6. with a pair of sterile gloves or forceps thread the catheter from its packet into the urethra. Ensure that
it is well into the bladder and the urine flowing.
7. inflate the retaining balloon according to manufacturer’s advice. 8. gently withdraw the catheter until resistance is felt. 9. connect to drainage bag. Sometimes an indwelling catheter is expelled by spasm, or because of a blockage or stone. Although a catheter with a larger size bulb is less likely to be expelled, the urethra can be damaged and permanently enlarged if the larger one is in turn expelled. If you have problems with an indwelling catheter, you should get advice from your spinal injuries centre. During periods, women may find that at the time of their menstrual period they tend to ‘leak’ around the catheter I have experienced difficulties achieving the best position on my leg to enable maximum drainage. A woman’s catheter is no use to me so I use a male catheter because of the longer length. Through my own research following advice from a community nurse experienced in catheter care, I have now managed to obtain the Simpla System, whereas before I was using mixed catheters and different makes of drainage bags. I think it important to mention that tetraplegics, because of low blood pressure, do not drain when in a sitting up position, but when in a recumbent position the urine drains freely, which is normally throughout the night. Suprapubic catheters
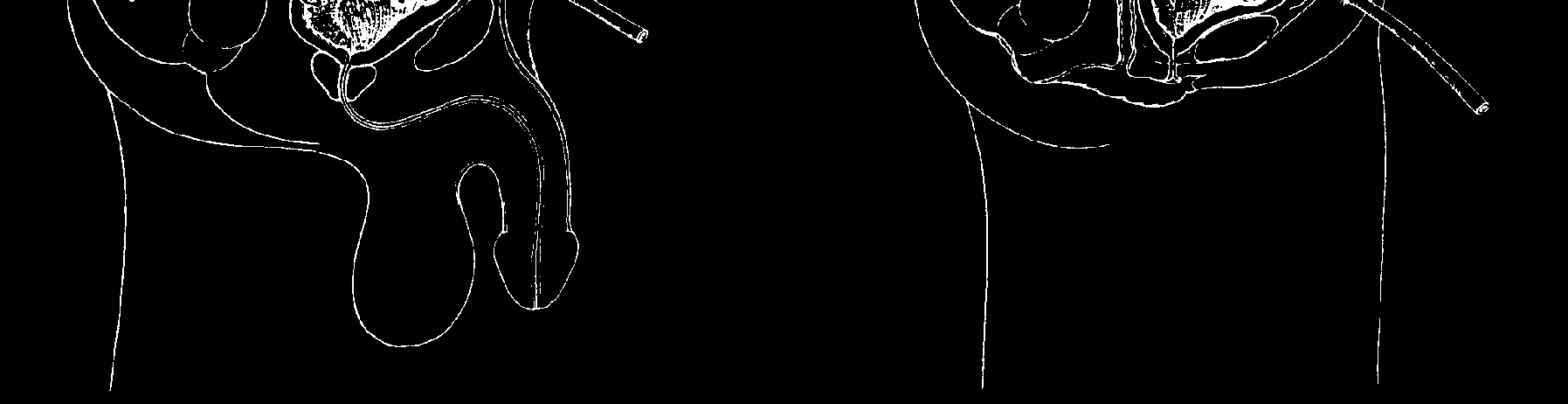
A suprapubic catheter is an indwelling catheter inserted into the bladder, bypassing the urethra, via a small surgical incision made just above the pubic area (see diagram on next page). It is sometimes used for newly injured people, and it is often used by women with reflex bladders, and people with acontractile bladders who do not have the manual dexterity to carry out intermittent self catheterisation. The catheter used is similar to that used for urethral use. It is changed in the same way as an indwelling urethral catheter. Hydrogel catheters are recommended for suprapubic use. 100% silicone catheters may be used with caution due to the occasional difficulty that is sometimes experienced on removal. The catheter should be changed every 4-6 weeks. The catheter should be taped to the lower abdomen and connected to a leg bag. A suprapubic catheter carries a similar risk of infection, blockage and stone formation as an indwelling urethral catheter, but protects and frees the private parts for sexual function. Because of the position of the opening, changing is easier than with a catheter passed through the urethra, especially for tetraplegics. Another advantage is there is less chance of the catheter tubing being sat on or kinked, and catheter changes can be carried out whilst sitting in a wheelchair. If the catheter becomes blocked urine may drain via the urethra, therefore reducing the risk of autonomic dysreflexia, but makes the patient wet. The incision is not permanent and closes on its own if it is later decided to manage the bladder by another method. I changed to the suprapubic catheter at the suggestion of the spinal unit and it is wonderful. I have the extra degree of independence of being able to change it when I want to and am not at the mercy of district nurses and continence advisers who are often at odds with the policies taught to you by the Spinal Unit. I welcomed the change as I had been experiencing problems with the urethral catheter for some years - I frequently rejected them (balloon still inflated) either due to spasms which had increased in intensity over the years or because I was passing a bladder stone - a condition I unfortunately developed during the last 7 years. Maybe I’ll pass enough to make a necklace! There are still stones with the new-style catheter, but they pass down the urethra without interfering with the catheter, and although I may get a little wet, I am not sitting in great puddles of urine as before. • Mrs D., Essex, C8/T1 complete The insertion of a suprapubic catheter may initially cause an increase in spasm. People with suprapubic catheters may experience oozing around the catheter site and this should be cleaned each day as part of your normal bathing routine. A dry gauze dressing may be applied each day.
Suprapubic catheter Male Female Bladder installation
Bladder installation should only be used if necessary. If your catheter consistently blocks with encrustations and requires frequent changing you may benefit from increasing your fluid intake and washing out your catheter with a solution. Prepacked sterile solutions can be prescribed by your GP. These vary from Saline solutions to acidic solutions. The frequency of use depends on how often catheters become blocked. It is advisable not to use acidic solutions more than once a week as they can irritate the bladder lining. It is best to warm the solution to reduce discomfort and spasm. Disconnect the catheter from the drainage bag, discard the bag and connect the sterile solution pack to the catheter. Gently squeeze the bag to push the fluid up into your bladder. Clamp the tube for the prescribed time (usually 20 minutes or so) and then release it, allowing the fluid to drain out. Bladder washout
Bladder washout should only be used if necessary. This is similar to a bladder instillation. However instead of a pre-packed sterile solution, a bladder syringe is used to inject fluid into your bladder. It is not common practice and advice should be sought from your spinal unit before attempting to carry out a bladder washout. If you have a urinary infection, care must be taken not to inject too much solution or too quickly, as this can carry the infection up to the kidneys. If anyone other than yourself performs the washout for you, they must wear sterile gloves. Use Milton or a similar solution to sterilise equipment. If you have an active bladder infection, take care not to inject too much solution or too rapidly, as fluid could carry the infection back up the ureters to the kidneys. 1. pour 300mls of sterile saline into a sterile jug; make sure it is not too hot or too cold. 2. disconnect the catheter from the drainage bag, discard the bag, and put the end of the catheter into
3. wash your hands or put on sterile gloves. 4. draw up 60mls of solution into a syringe. Inject into the bladder via the catheter with gentle but firm
pressure; wait 5 seconds, then withdraw the fluid slowly into the syringe.
5. disconnect the syringe from the catheter; don’t allow the end of the catheter to touch anything. 6. discard the used solution. 7. repeat (seeinstructions 4 - 6 above) until all the solution is used up. 8. reconnect the catheter to a new sterile drainage bag. 9. check to make sure that the urine begins to flow and no blood is present. Sheaths and condoms
This form of bladder management may be used by men with reflex bladders. A urinary sheath or condom is applied to the penis, attached by a plastic tube to a collecting bag which is strapped either to your leg or belly, or can be hung beside your bed or wheelchair. There are two main types. Each type is available in different sizes in width and in length to ensure the best fit. Also available are latex and non-latex hypoallergenic sheaths to reduce skin problems. Urinary sheaths are purpose made. They have a tube outlet at the end, are designed to resist twisting and tearing, and usually come with their own adhesive strip, or an adhesive coating on the inside of the sheath itself. Contraceptive - type condoms (unlubricated), used together with an adapter or ‘stud’ which is placed inside the rolled-up condom. Scissors are used to make a hole through the condom where the stud projects, and it is connected to a drainage tube. Special adhesive is brushed or sprayed onto the penis and the condom rolled down and pressed into place. The tubing is then connected to a collecting bag. A handy tip to avoid getting adhesive on your pubic hair and scrotum is to fold a tissue in four, cut the corner and fit it over the penis to make an ‘apron’. Fit a new sheath or condom daily, and try to give your penis a rest for 2 hours in every 24. During this time thoroughly wash with soap and water, especially under the foreskin. Your skin may be allergic to some condom adhesives and you will need to experiment to find one that suits you. Inspect your penis carefully, and stop using a sheath/condom immediately if there are any signs of a rash, pressure or broken skin. If skin is particularly sore it may be necessary to have an indwelling urethral catheter for a short period to allow the skin to heal. If you are heavy and have a large abdomen which ‘overhangs’ your penis, you may find it difficult or impossible to fit a sheath/condom and keep it in place. There is no real remedy other than to lose some weight. Some men might be suitable for the insertion of penile implants to allow a condom sheath to fit appropriately. A tip: some men use a strategically placed shaving mirror to help them apply the sheath. Tapping The reflex to empty the bladder can be triggered by tapping with the side of the hand at the base of the stomach, just above the pubic area; some people find it helpful to stroke the inside of the thighs or perineum (the area just in front of your anus), pull on their pubic hairs, or gently stretch the rectum with a finger. Nowadays it is not routinely recommended that you express the bladder by applying pressure over the lower abdomen, as it is felt to contribute to stress incontinence and reflux of urine to the kidneys. Because of the convenience and reliability of sheath/condom drainage systems, it is easy to forget your bladder training. Unless you ‘tap’ at regular intervals (every 3-4 hours) to ensure that the bladder is properly emptied, you will be prone to infections. Also, your bladder muscles will become ‘lazy’ and your bladder will gradually tend to retain increasing amounts of urine. Urinals
There are numerous different models, some in plastic, some in stainless steel. Some merely have a snap-on lid, but others have a no-spill adapter with a rubber sleeve which fits around the penis, and a non-return valve. Some are disposable. Contact your local Continence Advisor or Spinal Injury Centre for advice about the best one for you. Specifics for women
You may find that your bladder becomes much harder to control just before and during your period, and possibly also around the time of ovulation. Your difficulties may also increase during pregnancy, especially the later phases. Drainage bags
Urine drainage bags are connected to a condom or catheter by plastic tubing. Different bags can be worn on the upper or lower leg, across the stomach, or hung beside a bed or wheelchair. They can be disposable or reusable. Leg bags, with capacities from 350 to 1,300ml can be attached by straps or by a stocking-type sleeve. Overnight bags have larger capacities, up to two litres. Never lift a drainage bag above the level of the bladder, unless you are sure that your system has a well-functioning non-return valve! Continence supplies
To help you find out what’s available, we’ve included a list of companies that are frequently used by SIA members for catheters and continence products. Astra Tech Ltd, Stroud Water Business Park, Brunel Way, Stonehouse, Gloucester GL10 35W Tel: 01453 791763 Website: www.astratechuk.com Bard Ltd, Forest House, Brighton Road, Crawley, West Sussex RH11 9BP Tel: 01293 527888 Website: www.crbard.com C.S.Bullen Ltd, 3-7 Moss Street, Liverpool L6 1EY Tel: 0151 207 6995 Coloplast Ltd, Peterborough Business Park, Peterborough PE2 6FX Tel: 01733 392000 Website: www.coloplast.co.uk Jade-Euro-Med Ltd, Unit 14, East Hanningfield Industrial Estate, Old Church Road, East Henningfield, Chelmsford, Essex CM3 8BG Tel: 01245 400413 Manfred Sauer UK, Unit 3 IO Centre, Lodgefarm Industrial Estate, Northamption, NN5 7UW, Tel: 01604 588090 Website: www.legbags.com Simple Continence Care:A division of SSL International plc, Toft Hall, Knutsford, Cheshire WA16 9PD Tel: 0161 654 3000 SIMS Portex Ltd,Colonial Way, Watford, Herts, WD24 4LG. Tel: 01923 246 434 Website: www.smiths-medical.com
Who can help?
● Your spinal injuries unit is your first source of help and advice as they have a vast amount of
experience specifically accumulated with spinal cord injured people
• Your GP ● A Continence Advisor or nurse, employed by the local Trust may see you at a clinic or visit you at
home, and can usually tell you what equipment and supplies are available and where to get them
● The district (or community) nurse may help you with bladder and bowel care, and arrange supplies for
● Social Services or the Local Authority in some areas run a laundry service for soiled linen and/or
disposal service for soiled pads and bed pans.
I strongly advocate that the best people to deal with any problems are those linked to the spinal injury centre. Do not be dictated to by district nurses or incontinence advisers who are usually governed by the local health authority rules and not by what suits you as an individual. It’s your body, let it be known how you want things done. • Mrs D., Essex, C8/T1 complete
Drugs for bladder management
Various drugs are commonly prescribed to assist bladder management. Some of these are:
MEDICATIONS FOR BLADDER MANAGEMENT Function How they work
relax sphincter muscles and Prazosin (Hypovase) neck of bladder
* the ‘generic’ name is given first. Possible brand-name versions are given in brackets, but
there may be different names from other suppliers, as well as combination drugs
Urinary tract infections Fortunately, the signs of infection are usually clear: cloudy urine, often dark coloured and strong smelling, pink urine (however eating beetroot can also produce beautiful pink urine, and eating asparagus can make the urine smelly!), a decrease in the amount of urine passed, and an increase in mucus. Accompanying symptoms are an increase in spasm, high temperature, shivering and sweating. Infection in the bladder can pass up to the kidneys and damage them. Frequent infections can cause scarring of your bladder which may affect its ability to contract properly. At the first sign of a urinary tract infection, increase fluid intake and ensure your bladder is emptied frequently and completely. If you are ill or signs of infection persist contact your GP. Urinary tract infection is defined as a positive urine culture indicating the growth of bugs in the urine. There will also be flu-like symptoms including feeling unwell and running a temperature etc. NB; A positive culture on
its own, especially in the presence of a catheter is meaningless. There should always be symptoms of infection in order to justify the taking of antibiotics. Stones
Stones or calculi can develop in your kidneys and/or bladder. You are more prone to this after your injury because of your lower mobility, the loss of some calcium from the bones of your paralysed limbs (although this is usually limited to the months immediately after injury), and your less efficient bladder function. Smaller stones can be passed out through the bladder and urethra without your noticing. Larger ones can create obstruction in the kidney, or obstruct an indwelling catheter, and make you more susceptible to urinary tract infections. The symptoms are similar to those of a urinary tract infection, with greater difficulty in passing urine and more likelihood of pink-tinged urine (with blood in it). You will need treatment in hospital. Nowadays stones can often be broken up by ultrasound (lithotripsy) without the need for an operation or removed through an endoscope. Stone formation is best prevented by increasing your fluid intake (see above), cutting down on foods (especially milk and cheese) which are high in calcium,and trying to keep your urine acid). Bladder operations
Sphincterotomy - some men with ‘reflex’ bladders (most lesions T12 and above) may need a minor operation to cut the sphincter at the outlet of their bladder, as although their bladder reflexes work, they are not synchronised properly so that when their detrusor muscle (in the wall of the bladder) contracts to squeeze out the urine, the sphincter at the outlet of the bladder does not relax to allow bladder emptying. If left untreated, this condition leads to over-filling of the bladder and the risk of urine backing up to and infecting the kidneys. There is a small chance that the operation will affect the ability to obtain a reflex erection. It also might lead to disruption of ejaculation. This operation is not normally carried out on women. Bladder neck incision - in some men there is an obstruction at the neck of the bladder which needs a small incision to correct. This operation commonly leads to disruption of normal ejaculation if this existed before. Cystoplasty - this is an operation to enlarge the bladder and to reduce bladder activity by positioning a section of the bowel into it, or using the bladder wall itself to enlarge the bladder. Cystoscopy - this is a visual examination of the bladder by means of a tiny instrument inserted through the urethra. Feneley procedure - this is an uncommon operation performed on women to close the urethra and bladder neck and insert a suprapubic catheter. It is used when other methods of bladder management have failed and there is frequent leakage around an indwelling urethral catheter. Ileal conduit - now seldom used for spinal cord injured people, this is an operation to bypass the bladder completely. The ureters, which bring urine from the kidneys are diverted into a small pouch made from a section of the small intestine and thence by an opening in the abdomen to a removable external drainage bag. I had an ileal conduit done in September 1991. It was a last resort for me. I didn’t go through a spinal unit when I was injured, but spent the first year in a neurology ward. When I went home I had an indwelling catheter and I was never told there was any other option. I was sent to the spinal unit about five years after my injury as by this time I was having a lot of problems with my bladder. I was told it had shrivelled up and this was why it was going into spasm continuously and pushing out my catheter size 16 with 30mls of water [in the balloon]. I really wanted to do intermittent catheterisation, but when I tried it didn’t work for me as my bladder was damaged beyond repair. I was angry that the staff in the neurology ward didn’t send me to the spinal unit when I was well enough after my accident. I am sure if they had I wouldn’t have half the problems I do now. Since I had my ileal conduit, life has improved as I don’t have the worry I had before of my catheter bypassing and also of my bladder going into spasm regularly. • Margaret McEleny, T4 complete Mitrofanoff procedure - the appendix or a piece of bowel is fashioned to form a ‘channel’ between the bladder and the abdominal wall. The ‘channel’ contains a non-return valve to prevent urinary leakage. As the bladder fills pressure is applied to the channel so that leakage doesn’t occur and the person can catheterise as appropriate, through the abdominal wall. This procedure is commonly carried out with cystoplasty. Stamey colposuspension - this is almost the opposite of a sphincterotomy. It is an operation, performed on women, to tighten the bladder neck to make it more ‘water-tight’. Stents - a small metal mesh implant is inserted at the external sphincter. The sphincter remains slightly open and aids urinary drainage. Stress leakage surgery - e.g. macroplastique and collagen implants are injected around the bladder neck to make the bladder more ‘water tight’. Colposuspension surgery involves ‘hitching’ the bladder neck up to prevent urinary leakage. Implants Artificial Urinary Sphincter (AUS) - this is an inflatable cuff implanted around the neck of the bladder, with a control pump located in the scrotum or labia, and a balloon is placed in the abdomen. The cuff, which is filled with fluid, gently squeezes the bladder neck and urethra closed to keep urine in the bladder. When the pump is squeezed the fluid in the cuff flows into the balloon, allowing access to the bladder and drainage of urine. Within several minutes, fluid in the balloon automatically returns to the cuff, and the cuff again closes around the urethra. Carries some risk of infection. The average life span of an implanted artificial urinary sphincter is 10-12 years. This is because of the risk of infection and mechanical failures. Sacral Anterior Root Stimulator (SARS) - requires a major operation to install electrodes to stimulate the S2 to S4 anterior (front) nerve roots which control bladder function. These are connected to a tiny receiver block, installed beneath the skin below the rib cage. When you want to empty your bladder, you hold a small ‘transmitter’ control box up against your body. During the operation to implant the electrodes, the posterior (rear) nerve roots at the same level are usually severed permanently (‘posterior rhizotomy’), which is necessary to suppress reflex activity of the bladder (the main cause of incontinence in people with lesions T12 and above). The idea to sever some nerves might be disliked by some people. A SARS implant can achieve dramatic improvement in bladder continence and may also help bowel management. SARS operations have been performed worldwide, the majority on women, who have more to gain (because of their greater continence problems) and less to lose (some men may lose the ability to get a reflex erection as a result of the operation, though some do get good erections). Medical opinions about the costs and benefits of SARS differ. The operation is unsuitable for people with very low lesions (where the sacral segments of the spinal cord are damaged), those whose bladders have already been badly damaged, and those with incomplete lesions who retain pain sensitivity or good sensation in the genital area (which they are unlikely to want to forego). Tetraplegic women who cannot transfer to the toilet without assistance are unlikely to derive much benefit from the operation. To my great satisfaction and disbelief, I have not been wet since the day I had the operation. Neither have I had any complications as a result of having the implant. My bladder function continues to improve and I can sleep comfortably through the night without having to get up to use the loo at all. my bowel function is much more regular now and I have to take less laxatives than I used to. this operation has changed the quality of my life. • Susan Abbott, T10 The one disadvantage of increased spasm in my legs is one I am prepared to put up with, as the advantages far outweigh the disadvantages • Margaret Maugham, T11 Both the above SIA members had their SARS operations more than 10 years ago, and confirm that the benefits have continued, and that they have no regrets. Margaret Maughan recently had a minor operation to replace the receiver unit, but has had no further problems. For more bladder information go to www.spinal.co.uk and download the Bladder Factsheet in the Help & Advice zone. ‘Choosing Products for Bladder & Bowel Control’ is a guide to the most suitable products for adults with tips on choosing and using, complete with addresses. To order phone Ricability on 020 7427 2460. Also available on-line atwww.ricability.org.uk The Continence Foundation have a mass of leaflets and books covering most aspects of bladder management for very reasonable prices (50p a leaflet). For a full list of these phone the Foundation on 020 7404 6875. Or go to their comprehensive web site at www.continence-foundation.org.uk We are grateful to Wendy Pickard, Senior Clinical Nurse at the Outpatient Services at the Duke of Cornwall Spinal Treatment Centre for helping SIA with this text. SIA have checked with sources believed to be reliable in their efforts to provide information that is accurate, comprehensive, and timely at the date of publication. However, human error and changes can and will occur. The Spinal Injuries Association expressly disclaim any representation or warranty, expressed or implied, concerning the accuracy, comprehensiveness, or suitability of the information for a particular purpose. SIA have produced this document in good faith and are not responsible for any errors, omissions, or results obtained from the use of the information herein. • Bladder and Bowel Management for people with spinal cord injuries (2004 booklet) is available from SIA Price £5.00 The essentials of understanding the functioning of, and looking after one’s bladder and bowel after becoming spinal cord injured. This booklet is for the spinal cord injured person and anyone else who is involved in helping with this part of an SCI’s bodycare. It deals with the subject in a straightforward manner and looks at current practice both in hospital and at home.
SIA has checked with sources believed to be reliable in their efforts to provide information that is accurate, comprehensive, and timely at the date of publication. However, human error and changes can and will occur. The Spinal Injuries Association expressly disclaims any representation or warranty, expressed or implied, concerning the accuracy, comprehensiveness, or suitability of the information for a particular purpose. SIA has produced this document in good faith and is not responsible for any errors, omissions, or results obtained from the use of the information herein. Last Updated March 2006.
CME Renal Medicine on therapy in renal disease. Arch Intern Med 1981; 141 :1039–41. Richard S, Jothy S. A prospective study on Liam Plant MB MRCPI FRCPE, Consultant the impact of the renal biopsy in clinicalRenal Physician, Department of Renal management. Clin Nephrol 1986; 26 :217–21. 5 Cohen AH, Nast CC, Adler SG, Kopple JD. Medicine, Cork University Hospital, Cork, Clinica
STAFF REPORT General Manager, Shelter, Support and Housing Administration Purpose: This report updates Council on harm reduction and abstinence based programming in Toronto’s shelter system and responds to Council requests for information on the distribution of cigarettes and alcohol in shelter programs. Financial Implications and Impact Statement: There are no financial implications aris
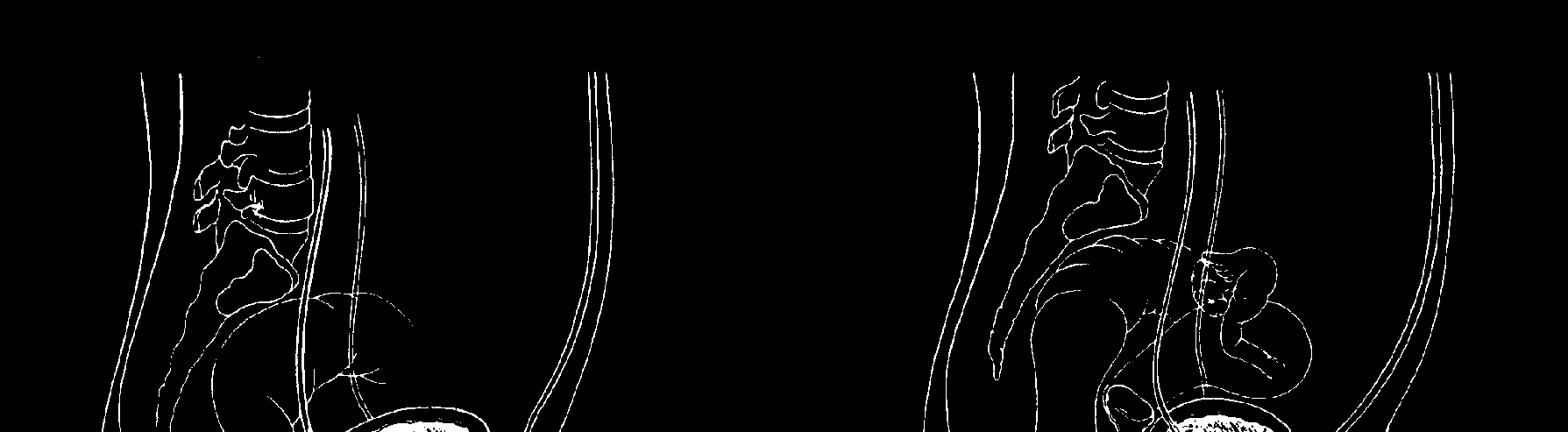
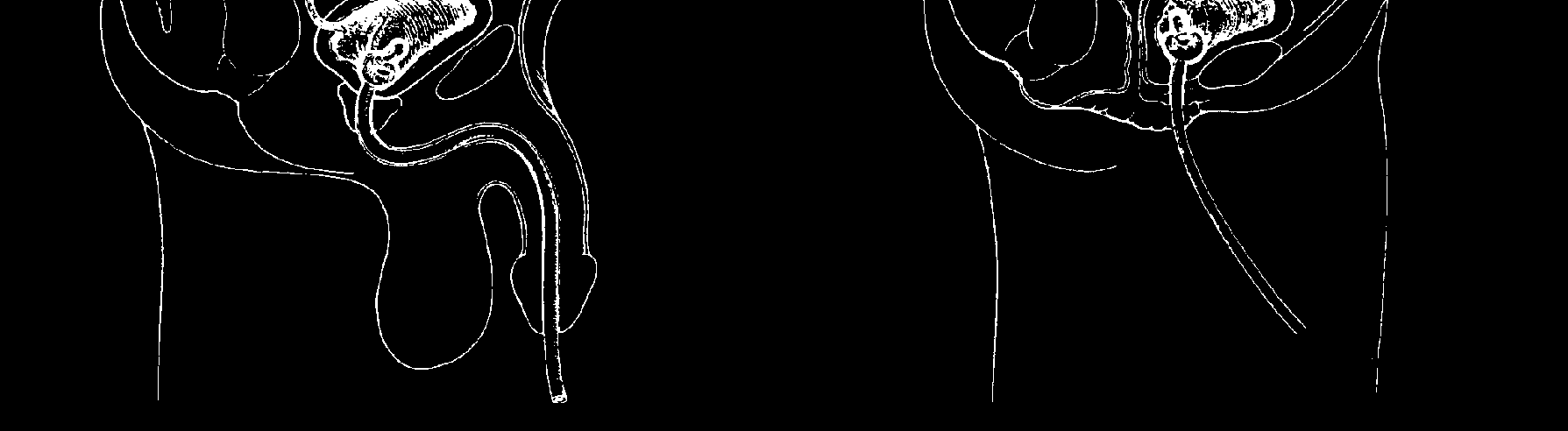 Indwelling catheter
Indwelling catheter 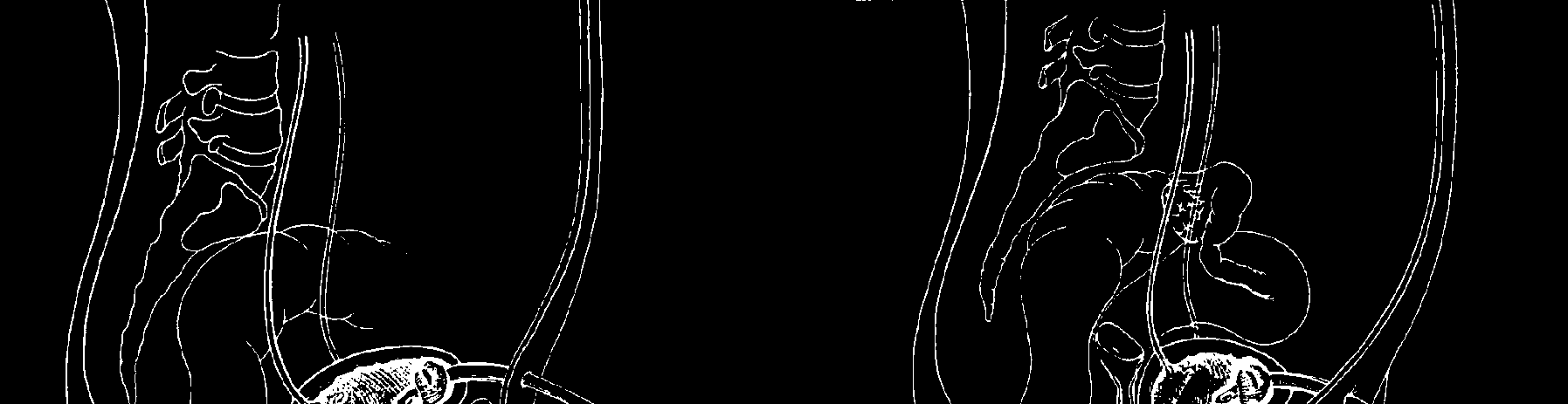
 Male Female
Male Female